

Relative cost and outcomes in the intensive care unit of acute lung injury (ALI) due to pandemic influenza compared with other etiologies: a single-center study
- PMID: 22929215
- PMCID: PMC3503790
- DOI: 10.1186/2110-5820-2-41
Relative cost and outcomes in the intensive care unit of acute lung injury (ALI) due to pandemic influenza compared with other etiologies: a single-center study
Abstract
Background: Critical illness due to 2009 H1N1 influenza has been characterized by respiratory complications, including acute lung injury (ALI) or acute respiratory distress syndrome (ARDS), and associated with high mortality. We studied the severity, outcomes, and hospital charges of patients with ALI/ARDS secondary to pandemic influenza A infection compared with ALI and ARDS from other etiologies.
Methods: A retrospective review was conducted that included patients admitted to the Cleveland Clinic MICU with ALI/ARDS and confirmed influenza A infection, and all patients admitted with ALI/ARDS from any other etiology from September 2009 to March 2010. An itemized list of individual hospital charges was obtained for each patient from the hospital billing office and organized by billing code into a database. Continuous data that were normally distributed are presented as the mean ± SD and were analyzed by the Student's t test. The chi-square and Fisher exact tests were used to evaluate differences in proportions between patient subgroups. Data that were not normally distributed were compared with the Wilcoxon rank-sum test.
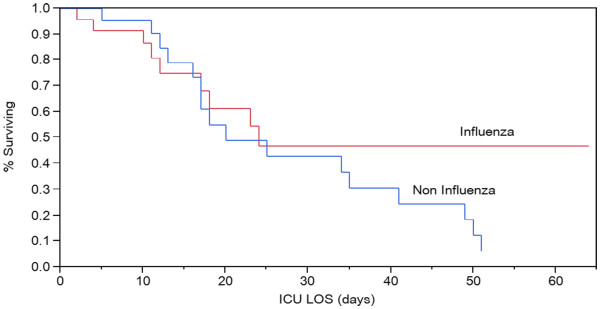
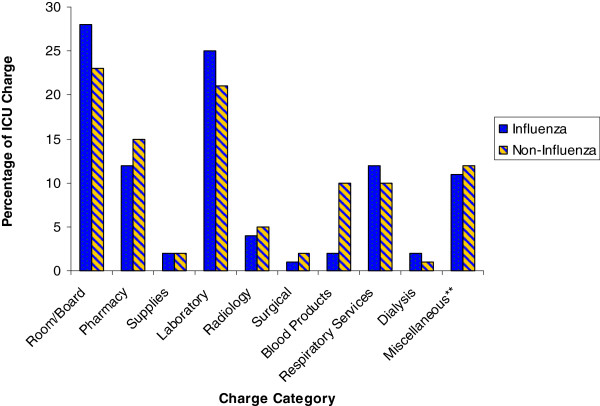
Results: Forty-five patients were studied: 23 in the H1N1 group and 22 in the noninfluenza group. Mean ± SD age was similar (44 ± 13 and 51 ± 17 years, respectively, p = 0.15). H1N1 patients had lower APACHE III scores (66 ± 20 vs. 89 ± 32, p = 0.015) and had higher Pplat and PEEP on days 1, 3, and 14. Hospital and ICU length of stay and duration of mechanical ventilation were comparable. SOFA scores over the first 2 weeks in the ICU indicate more severe organ failure in the noninfluenza group (p = 0.017). Hospital mortality was significantly higher in the noninfluenza group (77 vs. 39%, p = 0.016). The noninfluenza group tended to have higher overall charges, including significantly higher cost of blood products in the ICU.
Conclusions: ALI/ARDS secondary to pandemic influenza infection is associated with more severe respiratory compromise but has lower overall acuity and better survival rates than ALI/ARDS due to other causes. Higher absolute charges in the noninfluenza group are likely due to underlying comorbid medical conditions.
Figures
Similar articles
-
Etiology and outcomes of pulmonary and extrapulmonary acute lung injury/ARDS in a respiratory ICU in North India.Chest. 2006 Sep;130(3):724-9. doi: 10.1378/chest.130.3.724. Chest. 2006. PMID: 16963669
-
[Dynamic measurement of volume of atelectasis area in the evaluation of the prognosis of patients with moderate-to-severe acute respiratory distress syndrome].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Sep;32(9):1056-1060. doi: 10.3760/cma.j.cn121430-20191219-00056. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 33081890 Chinese.
-
Incidence of and Risk Factors for Acute Respiratory Distress Syndrome in Patients Admitted to Surgical Intensive Care Units: The Multicenter Thai University- Based Surgical Intensive Care Unit (THAI-SICU) Study.J Med Assoc Thai. 2016 Sep;99 Suppl 6:S118-S127. J Med Assoc Thai. 2016. PMID: 29906368
-
[Statin in the treatment of ALI/ARDS: a systematic review and Meta-analysis based on international databases].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Jan;29(1):51-56. doi: 10.3760/cma.j.issn.2095-4352.2017.01.011. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 28459404 Chinese.
-
[ARDS and influenza A (H1N1): patients' characteristics and management in intensive care unit. A literature review].Ann Fr Anesth Reanim. 2010 Feb;29(2):117-25. doi: 10.1016/j.annfar.2009.12.026. Epub 2010 Feb 8. Ann Fr Anesth Reanim. 2010. PMID: 20116970 Review. French.
Cited by
-
Real-Time Surveillance of Influenza Morbidity: Tracking Intensive Care Unit Resource Utilization.Ann Am Thorac Soc. 2017 Dec;14(12):1810-1817. doi: 10.1513/AnnalsATS.201609-721OC. Ann Am Thorac Soc. 2017. PMID: 28799774 Free PMC article.
-
Protective Effect of Seasonal Influenza Vaccination in Elderly Individuals with Disability in Taiwan: A Propensity Score-Matched, Nationwide, Population-Based Cohort Study.Vaccines (Basel). 2020 Mar 22;8(1):140. doi: 10.3390/vaccines8010140. Vaccines (Basel). 2020. PMID: 32235779 Free PMC article.
-
Critical illness associated with 2013-2014 influenza A (H1N1): Postpandemic characteristics, presentation and outcomes.Indian J Crit Care Med. 2015 Nov;19(11):636-41. doi: 10.4103/0972-5229.169328. Indian J Crit Care Med. 2015. PMID: 26730113 Free PMC article.
-
Using Incentives to Improve Resource Utilization: A Quasi-Experimental Evaluation of an ICU Quality Improvement Program.Crit Care Med. 2016 Jan;44(1):162-70. doi: 10.1097/CCM.0000000000001395. Crit Care Med. 2016. PMID: 26496444 Free PMC article.
-
Is omega-3 fatty acids enriched nutrition support safe for critical ill patients? A systematic review and meta-analysis.Nutrients. 2014 May 30;6(6):2148-64. doi: 10.3390/nu6062148. Nutrients. 2014. PMID: 24886987 Free PMC article.
References
-
- World now at the start of 2009 influenza pandemic. 2009. Available: http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6... [accessed 12/28, 2010]
-
- Influenza Investigators ANZIC, Webb SA, Pettila V. et al.Critical care services and H1N1 influenza in Australia and New Zealand. N Engl J Med. 2009;2009(361):1925–1934. - PubMed
-
- Davies A, Jones D. Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators et al.Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA. 2009;302:1888–1895. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
