

A scoring system for the prognosis and treatment of malignant bowel obstruction
- PMID: 22929404
- PMCID: PMC3792226
- DOI: 10.1016/j.surg.2012.07.009
A scoring system for the prognosis and treatment of malignant bowel obstruction
Abstract
Background: Malignant bowel obstruction is a common result of end-stage abdominal cancer that is a treatment dilemma for many physicians. Little has been reported predicting outcomes or determining the role of surgical intervention. We sought to review our experience with surgical and nonsurgical management of malignant bowel obstruction to identify predictors of 30-day mortality and of who would most likely benefit from surgical intervention.
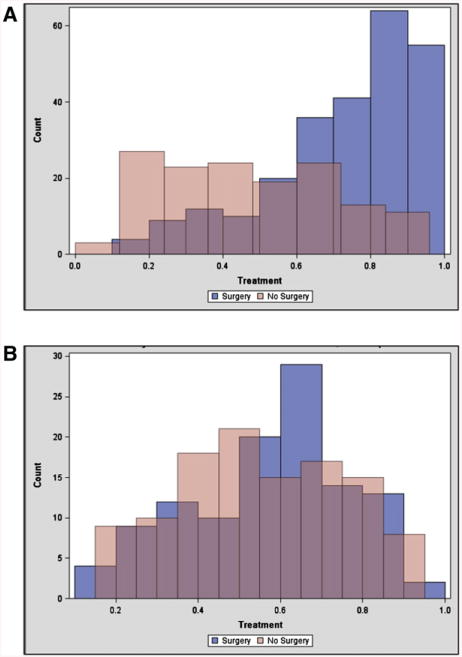
Methods: A chart review of 523 patients treated between 2000 and 2007 with malignant bowel obstruction were evaluated for factors present at admission to determine return to oral intake, 30-day mortality, and overall survival. Propensity score matching was used to homogenize patients treated with and without surgery to identify those who would benefit most from operative intervention.
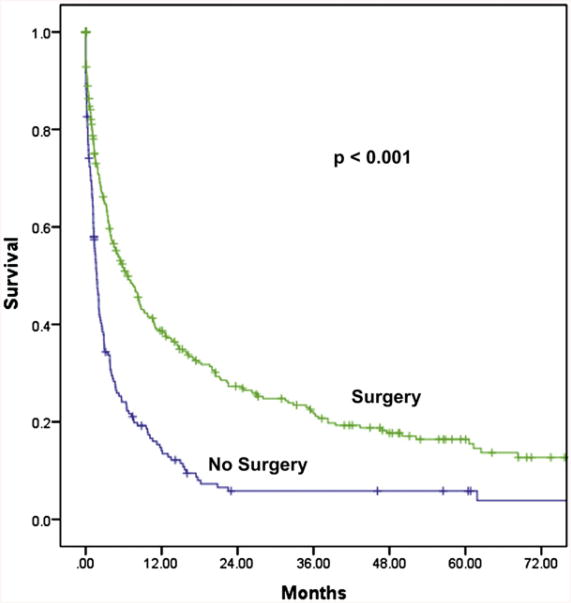
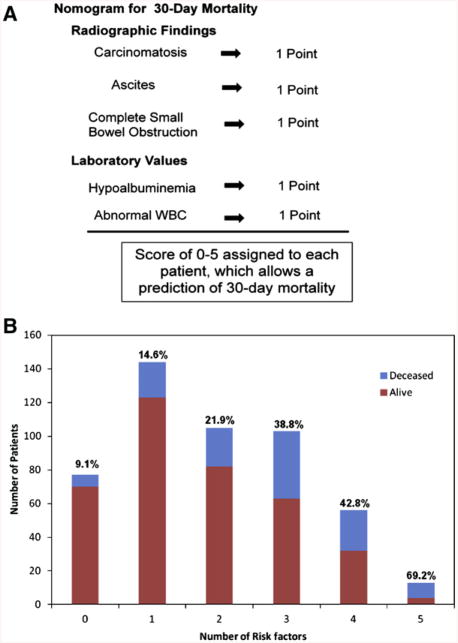
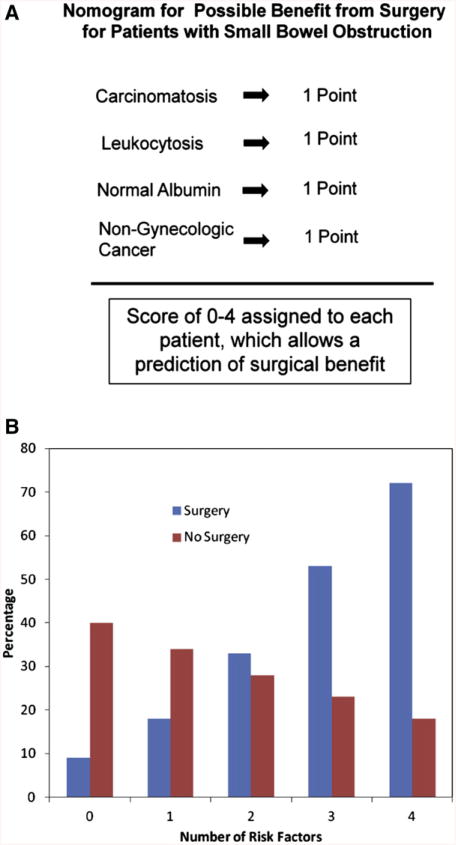
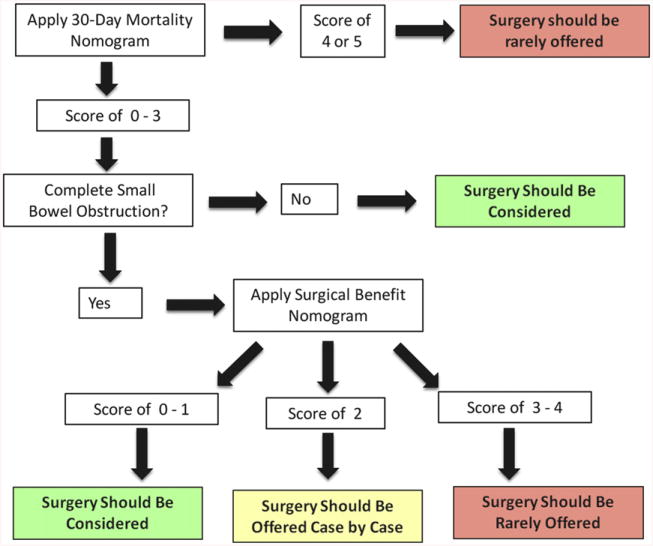
Results: Radiographic evidence of large bowel obstruction was predictive of return to oral intake. Hypoalbuminemia and radiographic evidence of ascites or carcinomatosis were all predictive of increased 30-day mortality and overall survival. A nomogram of 5 identified risk factors correlated with increased 30-day mortality independent of therapy. Patients with large bowel or partial small bowel obstruction benefited most from surgery. A second nomogram was created from 4 identified risk factors that revealed which patients with complete small bowel obstruction might benefit from surgery.
Conclusion: Two nomograms were created that may guide decisions in the care of patients with malignant bowel obstruction. These nomograms are able to predict 30-day mortality and who may benefit from surgery for small bowel obstruction.
Copyright © 2012 Mosby, Inc. All rights reserved.
Figures
References
-
- Dolan EA. Malignant bowel obstruction: a review of current treatment strategies. Am J Hosp Palliat Care. 2011;28:576–82. - PubMed
-
- Ripamonti C, Bruera E. Palliative management of malignant bowel obstruction. Int J Gynecol Cancer. 2002;12:135–43. - PubMed
-
- Ripamonti CI, Easson AM, Gerdes H. Management of malignant bowel obstruction. Eur J Cancer. 2008;44:1105–15. - PubMed
-
- Wong TH, Tan YM. Surgery for the palliation of intestinal obstruction in advanced abdominal malignancy. Singapore Med J. 2009;50:1139–44. - PubMed
-
- Selby D, Wright F, Stilos K, Daines P, Moravan V, Gill A, et al. Room for improvement? A quality-of-life assessment in patients with malignant bowel obstruction. Palliat Med. 2010;24:38–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
