

Establishing a murine model of the hematopoietic syndrome of the acute radiation syndrome
- PMID: 22929467
- PMCID: PMC3743168
- DOI: 10.1097/HP.0b013e3182667309
Establishing a murine model of the hematopoietic syndrome of the acute radiation syndrome
Abstract
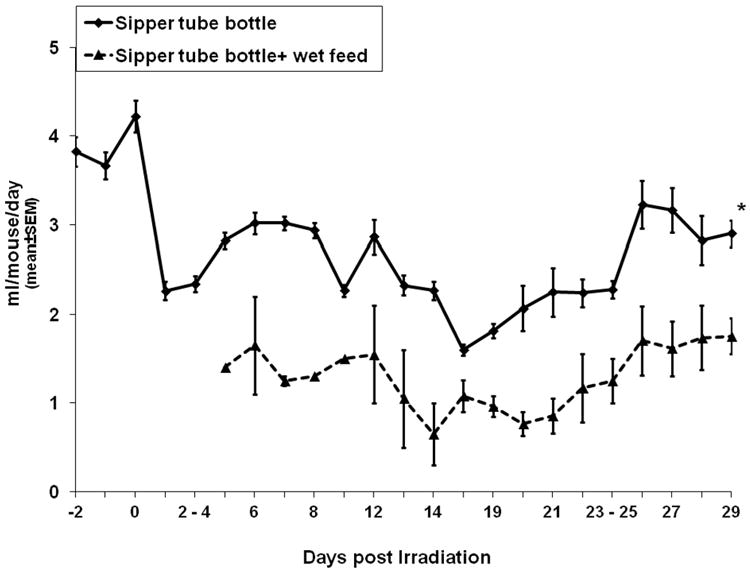
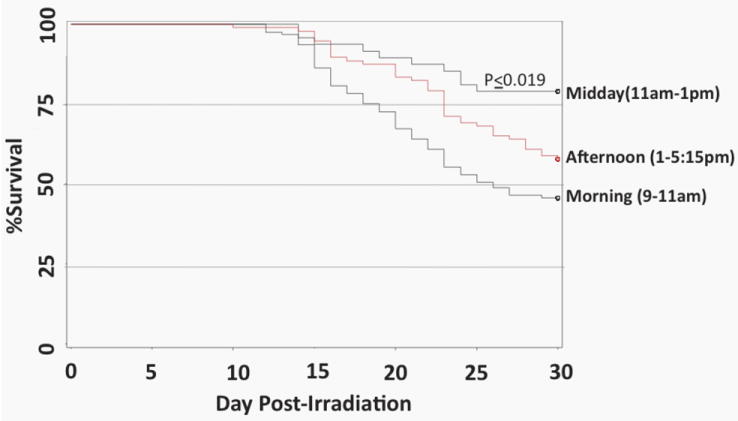
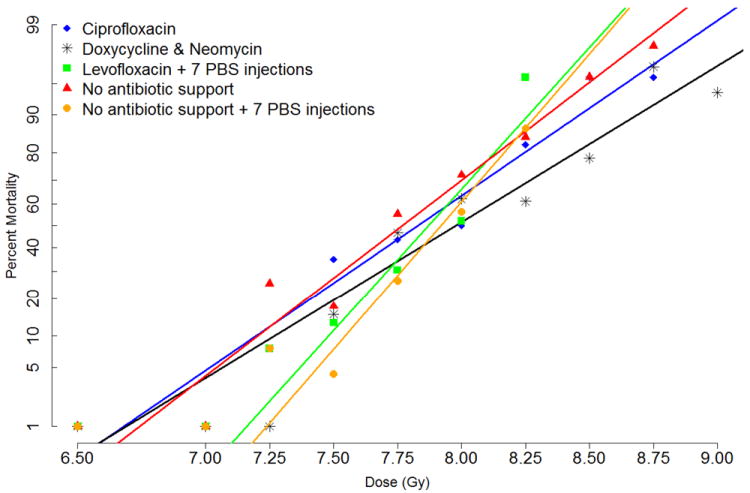
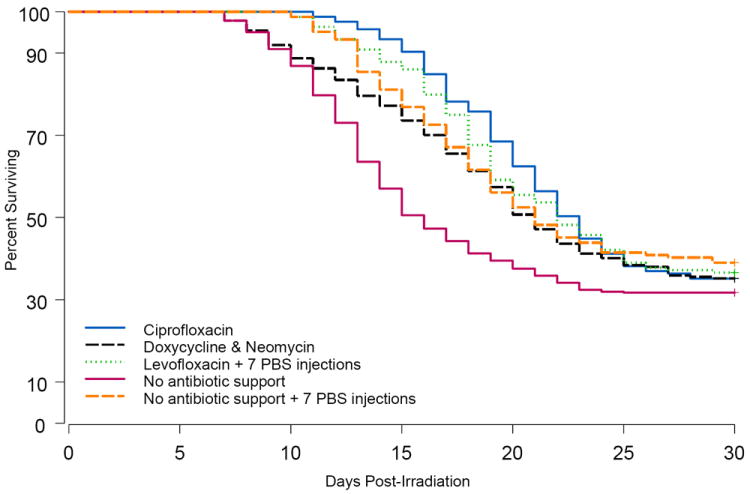
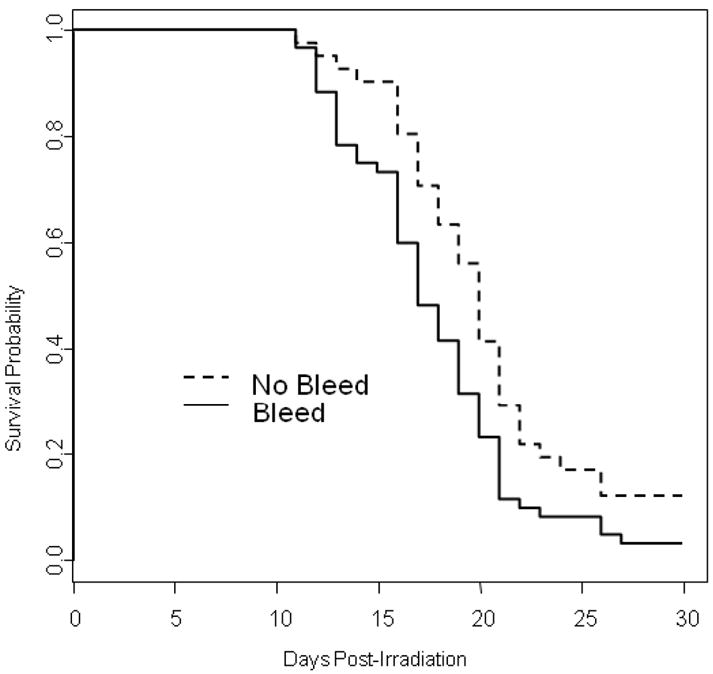
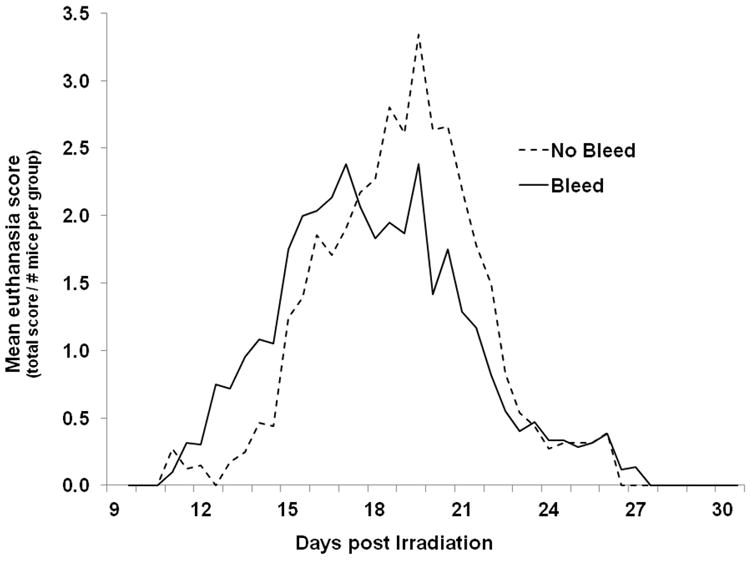
The authors have developed a murine model of the Hematopoietic Syndrome of the Acute Radiation Syndrome (H-ARS) for efficacy testing of medical countermeasures (MCM) against radiation according to the FDA Animal Rule. Ten- to 12-wk-old male and female C57BL/6 mice were exposed to the LD50/30-LD70/30 dose of total body irradiation (TBI, (137)Cs, 0.62-0.67 Gy min(-1)) in the morning hours when mice were determined to be most radiosensitive, and they were assessed for 30-d survival and mean survival time (MST). Antibiotics were delivered in drinking water on days 4-30 post-TBI at a concentration based on the amount of water that lethally-irradiated mice were found to consume. The fluoroquinolones, ciprofloxacin and levofloxacin, as well as the tetracycline doxycycline, and aminoglycoside neomycin, all significantly increased MST of decedent mice, while ciprofloxacin (p = 0.061) and doxycycline + neomycin (p = 0.005) showed at least some efficacy to increase 30-d survival. Blood sampling (30 μL/mouse every fifth day) was found to negatively impact 30-d survival. Histopathology of tissues harvested from nonmoribund mice showed expected effects of lethal irradiation, while moribund mice were largely septicemic with a preponderance of enteric organisms. Kinetics of loss and recovery of peripheral blood cells in untreated mice and those treated with two MCM, granulocyte-colony stimulating factor and Amifostine further characterized and validated this model for use in screening studies and pivotal efficacy studies of candidate MCM for licensure to treat irradiated individuals suffering from H-ARS.
Conflict of interest statement
No financial conflict of interest was declared by any of the authors.
Figures

References
-
- Anno GH, Young RW, Bloom RM, Mercier JR. Dose response relationships for acute ionizing-radiation lethality. Health Phys. 2003;84:565–75. - PubMed
-
- Baverstock K, Ash P. A review of radiation accidents involving whole body exposure and the relevance to the LD50/60for man. Br J Radiol. 1983;56:837. - PubMed
-
- Bishop MR, Tarantolo SR, Geller RB, Lynch JC, Bierman PJ, Pavletic ZS, Vose JM, Kruse S, Dix SP, Morris ME, Armitage JO, Kessinger A. A randomized, double-blind trial of filgrastim (granulocyte colony-stimulating factor) versus placebo following allogeneic blood stem cell transplantation. Blood. 2000;96:80–5. - PubMed
-
- Brook I, Elliott TB. Quinolone therapy in the prevention of mortality after irradiation. Radiat Res. 1991;128:100–3. - PubMed
-
- Brook I, Elliott TB, Ledney GD. Quinolone therapy of Klebsiella pneumoniae sepsis following irradiation: comparison of pefloxacin, ciprofloxacin, and ofloxacin. Radiat Res. 1990;122:215–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
