

The influence of device position on the flow within the Penn State 12 cc pediatric ventricular assist device
- PMID: 22929894
- PMCID: PMC3431512
- DOI: 10.1097/MAT.0b013e3182639a18
The influence of device position on the flow within the Penn State 12 cc pediatric ventricular assist device
Abstract
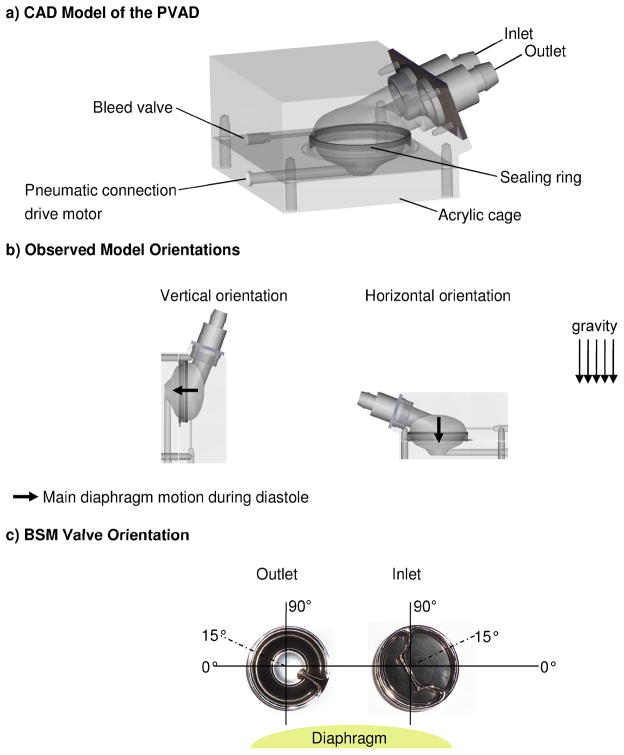
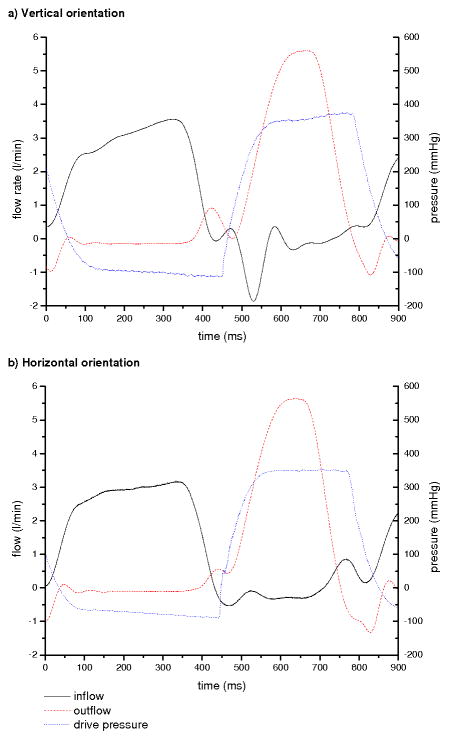
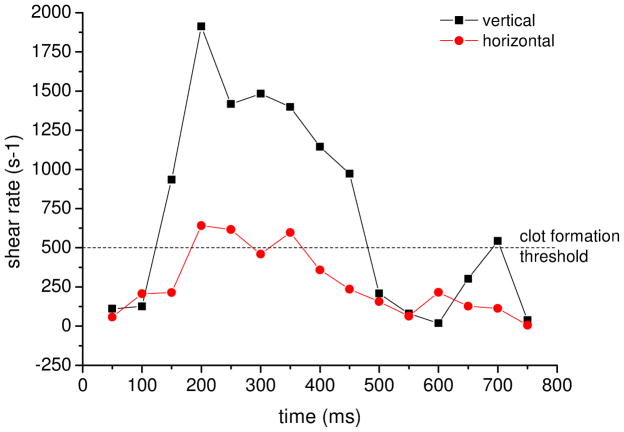
Ventricular assist devices are a commonly used heart failure therapy for adult patients as bridge-to-transplant or bridge-to-recovery tools. The application of adult ventricular assist devices in pediatric patients has led to increased thrombotic events. Therefore, we have been developing a pediatric ventricular assist device (PVAD), the Penn State 12 cc PVAD. It is designed for patients with a body weight of 5-15 kg and has a stroke volume of 12 cc. Clot formation is the major concern. It is correlated to the coagulability of blood, the blood contacting materials and the fluid dynamics within the system. The intent is for the PVAD to be a long term therapy. Therefore, the system may be oriented in different positions according to the patient's behavior. This study evaluates for the first time the impact of position on the flow patterns within the Penn State 12 cc PVAD, which may help to improve the PVAD design concerning chamber and ports geometries. The fluid dynamics are visualized by particle image velocimetry. The evaluation is based on inlet jet behavior and calculated wall shear rates. Vertical and horizontal model orientations are compared, both with a beat rate of 75, outlet pressures of 90/60 mm Hg and a flow rate of 1.3 l/min. The results show a significant change of the inlet jet behavior and the development of a rotational flow pattern. Vertically, the inlet jet is strong along the wall. It initiates a rotational flow pattern with a wandering axis of rotation. In contrast, the horizontal model orientation results show a weaker inlet jet along the wall with a nearly constant center of rotation location, which can be correlated to a higher risk of thrombotic events. In addition, high speed videography illustrates differences in the diaphragm motion during diastole. Diaphragm opening trajectories measurements determine no significant impact of the density of the blood analog fluids. Hence, the results correlate to human blood.
Figures










Similar articles
-
A parametric study of valve orientation on the flow patterns of the Penn State pulsatile pediatric ventricular assist device.ASAIO J. 2010 Jul-Aug;56(4):356-63. doi: 10.1097/MAT.0b013e3181e3cb22. ASAIO J. 2010. PMID: 20559131
-
Flow behavior within the 12-cc Penn State pulsatile pediatric ventricular assist device: an experimental study of the initial design.Artif Organs. 2008 Jun;32(6):442-52. doi: 10.1111/j.1525-1594.2008.00565.x. Epub 2008 Apr 16. Artif Organs. 2008. PMID: 18422800
-
Continuous and Pulsatile Pediatric Ventricular Assist Device Hemodynamics with a Viscoelastic Blood Model.Cardiovasc Eng Technol. 2016 Mar;7(1):23-43. doi: 10.1007/s13239-015-0252-8. Epub 2015 Dec 7. Cardiovasc Eng Technol. 2016. PMID: 26643646 Free PMC article.
-
The 12 cc Penn State pulsatile pediatric ventricular assist device: fluid dynamics associated with valve selection.J Biomech Eng. 2008 Aug;130(4):041019. doi: 10.1115/1.2939342. J Biomech Eng. 2008. PMID: 18601461
-
Review of recent results using computational fluid dynamics simulations in patients receiving mechanical assist devices for end-stage heart failure.Methodist Debakey Cardiovasc J. 2014 Jul-Sep;10(3):185-9. doi: 10.14797/mdcj-10-3-185. Methodist Debakey Cardiovasc J. 2014. PMID: 25574347 Free PMC article. Review.
Cited by
-
Effect of Hematocrit and Elevated Beat Rate on the 12cc Penn State Pediatric Ventricular Assist Device.ASAIO J. 2023 Dec 1;69(12):1065-1073. doi: 10.1097/MAT.0000000000002028. Epub 2023 Aug 7. ASAIO J. 2023. PMID: 37549654 Free PMC article.
-
Technology landscape of pediatric mechanical circulatory support devices: A systematic review 2010-2021.Artif Organs. 2022 Aug;46(8):1475-1490. doi: 10.1111/aor.14242. Epub 2022 Apr 14. Artif Organs. 2022. PMID: 35357020 Free PMC article.
-
Design of a pulsatile flow facility to evaluate thrombogenic potential of implantable cardiac devices.J Biomech Eng. 2015 Apr;137(4):045001. doi: 10.1115/1.4029579. Epub 2015 Feb 11. J Biomech Eng. 2015. PMID: 25587891 Free PMC article.
-
Fluid Dynamic Study of the Penn State Pediatric Total Artificial Heart.J Biomech Eng. 2024 Oct 1;146(10):101007. doi: 10.1115/1.4065377. J Biomech Eng. 2024. PMID: 38652582
-
Toward the Virtual Benchmarking of Pneumatic Ventricular Assist Devices: Application of a Novel Fluid-Structure Interaction-Based Strategy to the Penn State 12 cc Device.J Biomech Eng. 2017 Aug 1;139(8):0810081-08100810. doi: 10.1115/1.4036936. J Biomech Eng. 2017. PMID: 28586917 Free PMC article.
References
-
- Spillner J, Kopp R, Finocchiaro T, et al. Assisted circulation. an overview from a clinical perspective. Biomed Tech. 2009;54:255–267. - PubMed
-
- He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in US men and women. NHANES I epidemiologic follow-up study. Arch Intern Med. 2001;161:996–1002. - PubMed
-
- American Heart Association. Statistical Reference Book. Texas: 2005.
-
- Fynn-Thompson F, Almond C. Pediatric Ventricular Assist Devices. Pediatr Cardiol. 2007;28:149–155. - PubMed
-
- Hoffman JI, Kaplan S. The Incidence of Congenital Heart Disease. J Am Coll Cardiol. 2002;39:1890–1900. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
