

Self-reported gait unsteadiness in mildly impaired neurological patients: an objective assessment through statistical gait analysis
- PMID: 22931488
- PMCID: PMC3480904
- DOI: 10.1186/1743-0003-9-64
Self-reported gait unsteadiness in mildly impaired neurological patients: an objective assessment through statistical gait analysis
Abstract
Background: Self-reported gait unsteadiness is often a problem in neurological patients without any clinical evidence of ataxia, because it leads to reduced activity and limitations in function. However, in the literature there are only a few papers that address this disorder. The aim of this study is to identify objectively subclinical abnormal gait strategies in these patients.
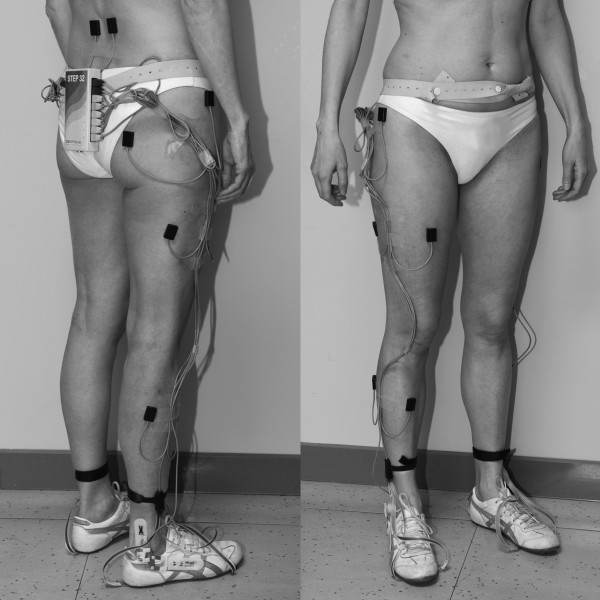
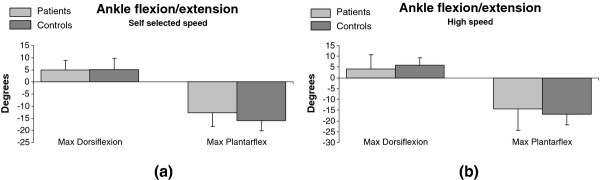
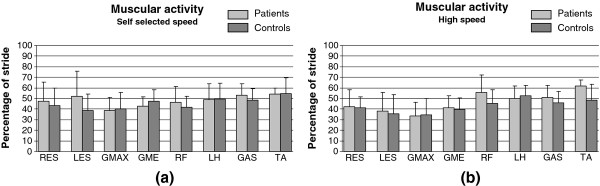
Methods: Eleven patients affected by self-reported unsteadiness during gait (4 TBI and 7 MS) and ten healthy subjects underwent gait analysis while walking back and forth on a 15-m long corridor. Time-distance parameters, ankle sagittal motion, and muscular activity during gait were acquired by a wearable gait analysis system (Step32, DemItalia, Italy) on a high number of successive strides in the same walk and statistically processed. Both self-selected gait speed and high speed were tested under relatively unconstrained conditions. Non-parametric statistical analysis (Mann-Whitney, Wilcoxon tests) was carried out on the means of the data of the two examined groups.
Results: The main findings, with data adjusted for velocity of progression, show that increased double support and reduced velocity of progression are the main parameters to discriminate patients with self-reported unsteadiness from healthy controls. Muscular intervals of activation showed a significant increase in the activity duration of the Rectus Femoris and Tibialis Anterior in patients with respect to the control group at high speed.
Conclusions: Patients with a subjective sensation of instability, not clinically documented, walk with altered strategies, especially at high gait speed. This is thought to depend on the mechanisms of postural control and coordination. The gait anomalies detected might explain the symptoms reported by the patients and allow for a more focused treatment design. The wearable gait analysis system used for long distance statistical walking assessment was able to detect subtle differences in functional performance monitoring, otherwise not detectable by common clinical examinations.
Figures
Similar articles
-
Temporospatial characteristics of gait in patients with lower limb muscle hypertonia after traumatic brain injury.Brain Inj. 2010;24(13-14):1575-84. doi: 10.3109/02699052.2010.523053. Epub 2010 Oct 25. Brain Inj. 2010. PMID: 20973631
-
Magnitude and variability of gait characteristics when walking on an irregular surface at different speeds.Hum Mov Sci. 2018 Jun;59:112-120. doi: 10.1016/j.humov.2018.04.003. Epub 2018 Apr 10. Hum Mov Sci. 2018. PMID: 29653340
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
-
Test-retest reliability and minimal detectable change of ankle kinematics and spatiotemporal parameters in MS population.Gait Posture. 2019 Oct;74:218-222. doi: 10.1016/j.gaitpost.2019.09.015. Epub 2019 Sep 16. Gait Posture. 2019. PMID: 31561120
-
Office management of gait disorders in the elderly.Can Fam Physician. 2011 Jul;57(7):765-70. Can Fam Physician. 2011. PMID: 21753097 Free PMC article. Review.
Cited by
-
Dual task-related gait changes in patients with mild cognitive impairment.Funct Neurol. 2015 Jan-Mar;30(1):59-65. Funct Neurol. 2015. PMID: 26214028 Free PMC article.
-
Muscle synergies in Parkinson's disease before and after the deep brain stimulation of the bilateral subthalamic nucleus.Sci Rep. 2023 Apr 28;13(1):6997. doi: 10.1038/s41598-023-34151-6. Sci Rep. 2023. PMID: 37117317 Free PMC article.
-
Atypical Gait Cycles in Parkinson's Disease.Sensors (Basel). 2021 Jul 27;21(15):5079. doi: 10.3390/s21155079. Sensors (Basel). 2021. PMID: 34372315 Free PMC article.
-
Acute Thermoregulatory and Cardiovascular Response to Submaximal Exercise in People With Multiple Sclerosis.Front Immunol. 2022 Jul 6;13:842269. doi: 10.3389/fimmu.2022.842269. eCollection 2022. Front Immunol. 2022. PMID: 35874684 Free PMC article.
-
Quantification of Axial Abnormality Due to Cerebellar Ataxia with Inertial Measurements.Sensors (Basel). 2018 Aug 24;18(9):2791. doi: 10.3390/s18092791. Sensors (Basel). 2018. PMID: 30149564 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
