

Right ventricular structure is associated with the risk of heart failure and cardiovascular death: the Multi-Ethnic Study of Atherosclerosis (MESA)--right ventricle study
- PMID: 22932258
- PMCID: PMC3532921
- DOI: 10.1161/CIRCULATIONAHA.112.095216
Right ventricular structure is associated with the risk of heart failure and cardiovascular death: the Multi-Ethnic Study of Atherosclerosis (MESA)--right ventricle study
Abstract
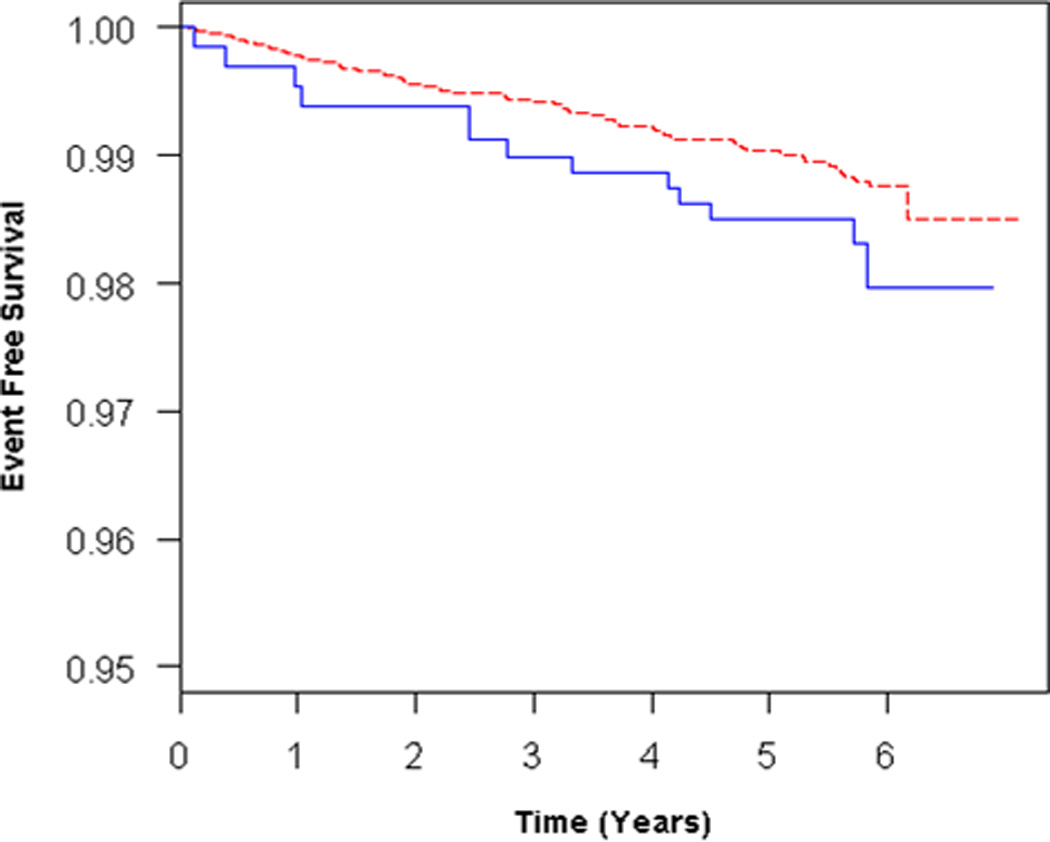
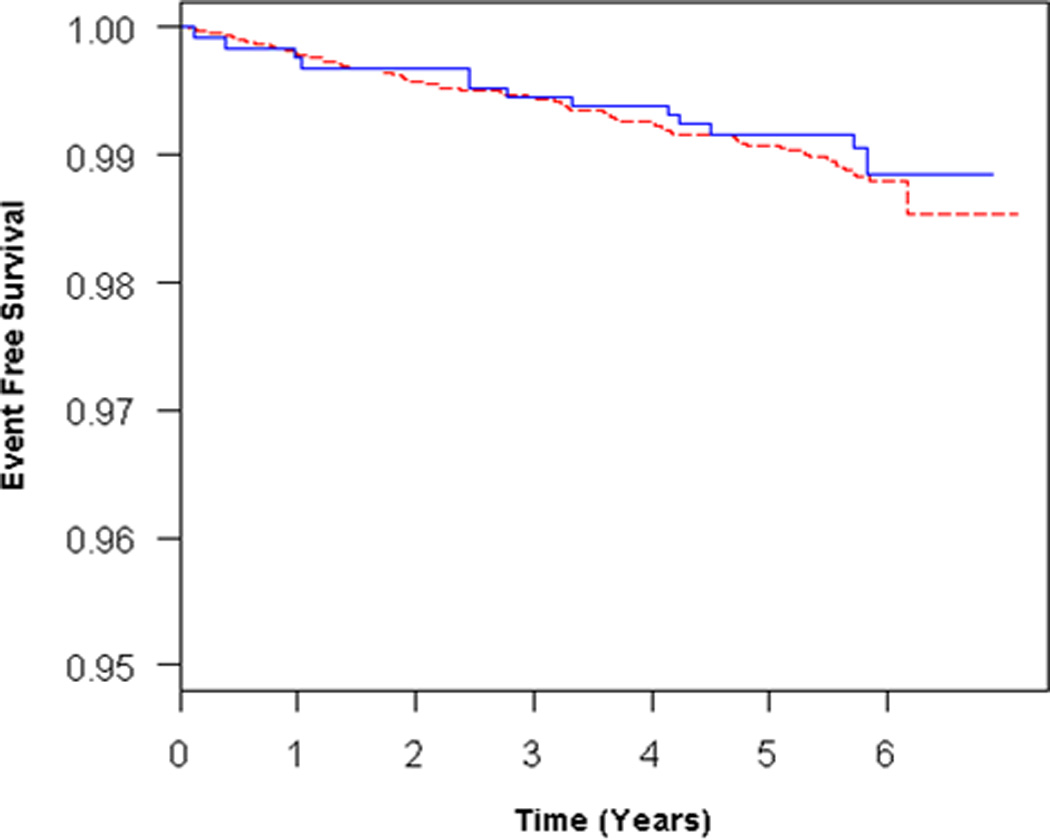
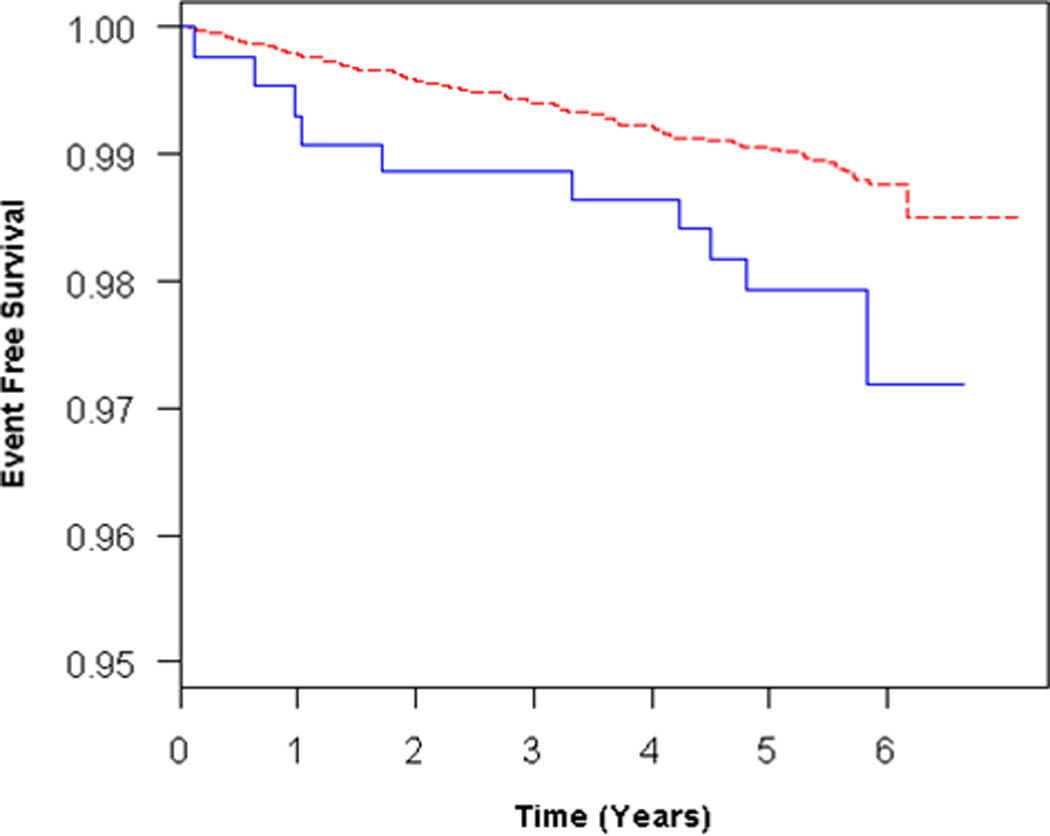
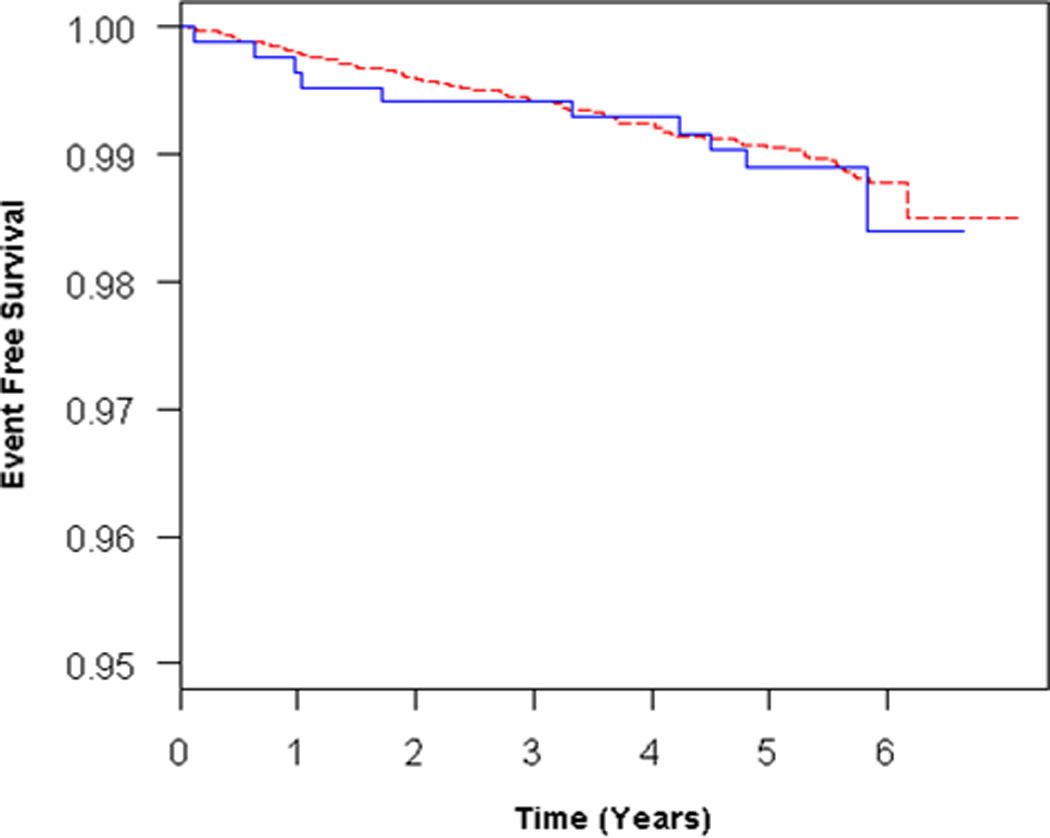
Background: Changes in right ventricular (RV) morphology are associated with morbidity and mortality in heart and lung disease. We examined the association of abnormal RV structure and function with the risk of heart failure or cardiovascular death in a population-based multiethnic sample free of clinical cardiovascular disease at baseline.
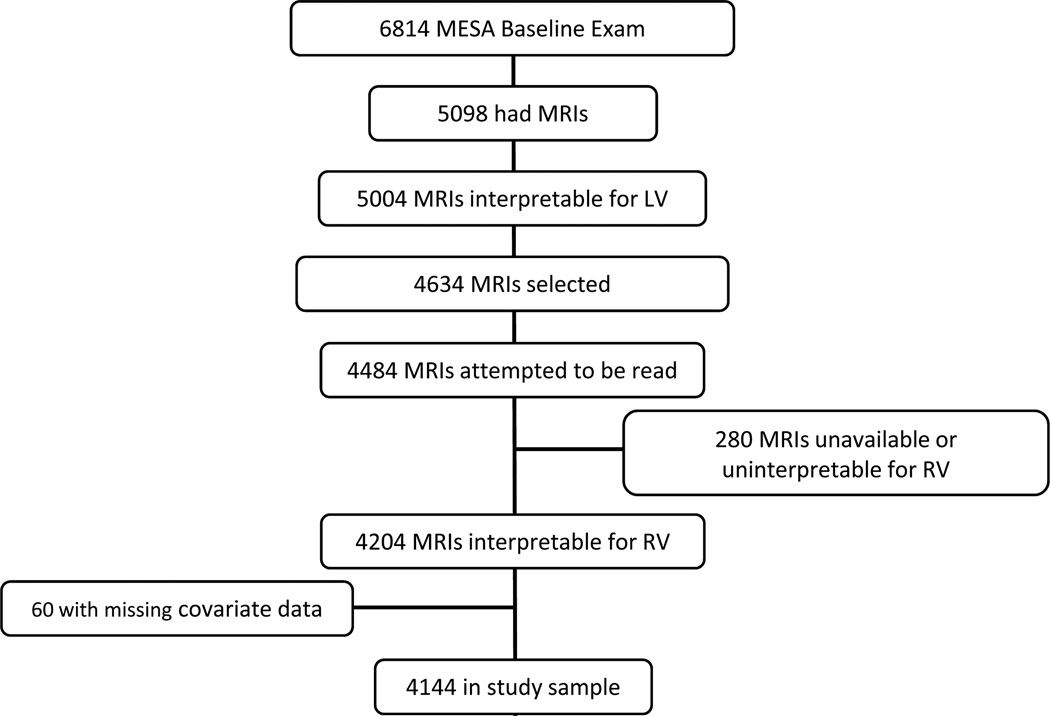
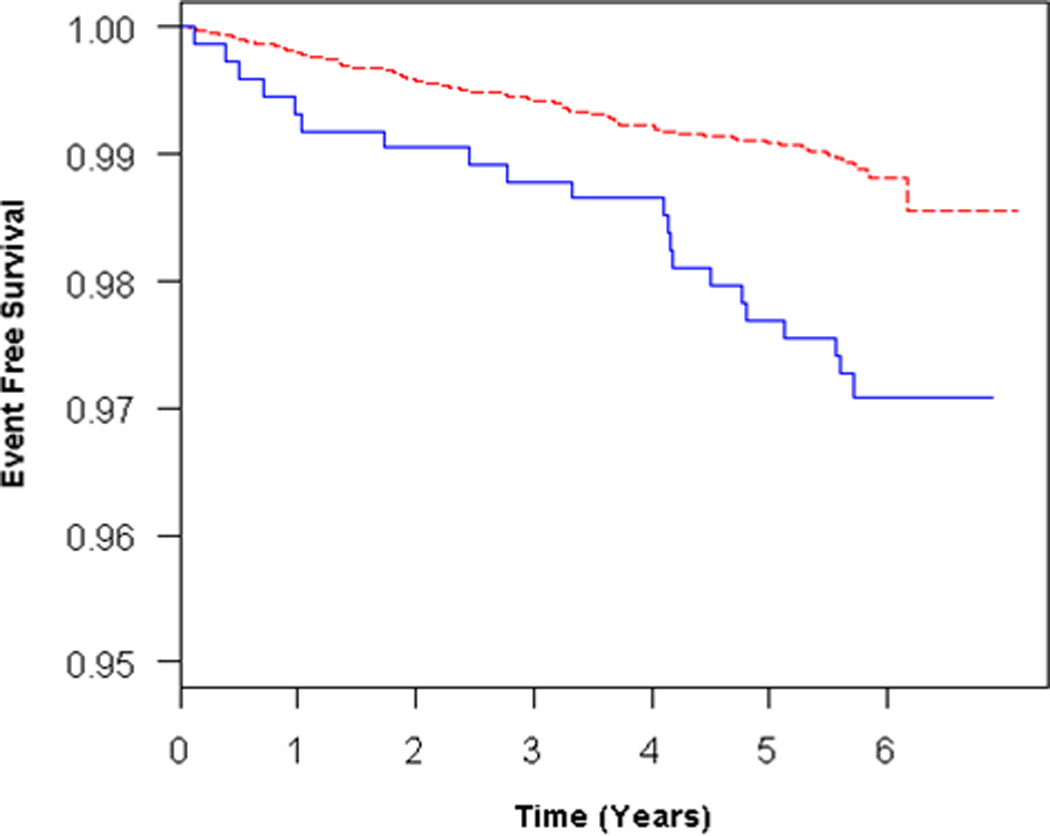
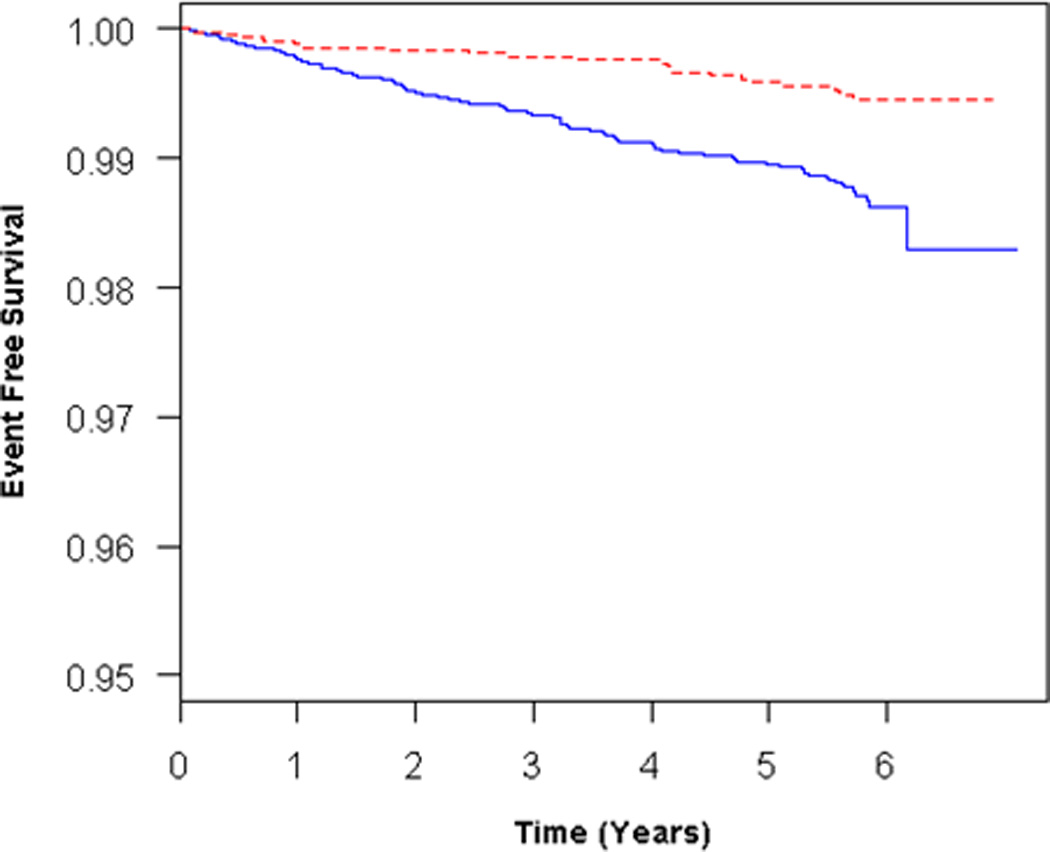
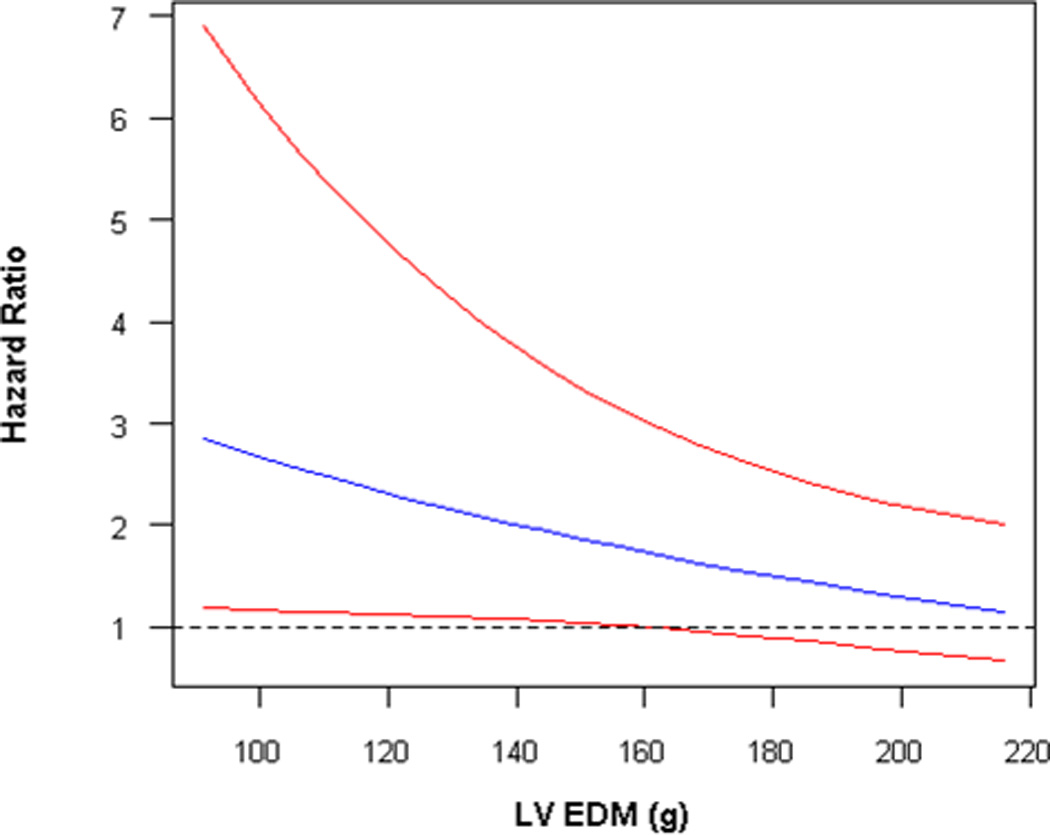
Methods and results: The Multi-Ethnic Study of Atherosclerosis (MESA) performed cardiac magnetic resonance imaging on 5098 participants between 2000 and 2002 with follow-up for incident heart failure and cardiovascular death ("death") until January 2008. RV volumes and mass were available for 4204 participants. The study sample (n=4144) was 61.4±10.1 years old and 47.6% male. The presence of RV hypertrophy (increased RV mass) was associated with more than twice the risk of heart failure or death after adjustment for demographics, body mass index, education, C-reactive protein level, hypertension, and smoking status (hazard ratio, 2.52; 95% confidence interval, 1.55-4.10; P<0.001) and a doubling (or more) of risk with left ventricular mass at the mean value or lower (P for interaction=0.05).
Conclusions: RV hypertrophy was associated with the risk of heart failure or death in a multiethnic population free of clinical cardiovascular disease at baseline.
Figures
Comment in
-
Hearing the right heart's sotto voce.Circulation. 2012 Oct 2;126(14):1673-5. doi: 10.1161/CIRCULATIONAHA.112.136598. Epub 2012 Aug 29. Circulation. 2012. PMID: 22932259 No abstract available.
References
-
- Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008;117:1717–1731. - PubMed
-
- Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117:1436–1448. - PubMed
-
- Kawut SM, Horn EM, Berekashvili KK, Garofano RP, Goldsmith RL, Widlitz AC, Rosenzweig EB, Kerstein D, Barst RJ. New predictors of outcome in idiopathic pulmonary arterial hypertension. Am J Cardiol. 2005;95:199–203. - PubMed
-
- van Wolferen SA, Marcus JT, Boonstra A, Marques KM, Bronzwaer JG, Spreeuwenberg MD, Postmus PE, Vonk-Noordegraaf A. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. Eur Heart J. 2007;28:1250–1257. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
