

Trevo versus Merci retrievers for thrombectomy revascularisation of large vessel occlusions in acute ischaemic stroke (TREVO 2): a randomised trial
- PMID: 22932714
- PMCID: PMC4176618
- DOI: 10.1016/S0140-6736(12)61299-9
Trevo versus Merci retrievers for thrombectomy revascularisation of large vessel occlusions in acute ischaemic stroke (TREVO 2): a randomised trial
Erratum in
- Lancet. 2012 Oct 6;380(9849):1230
Abstract
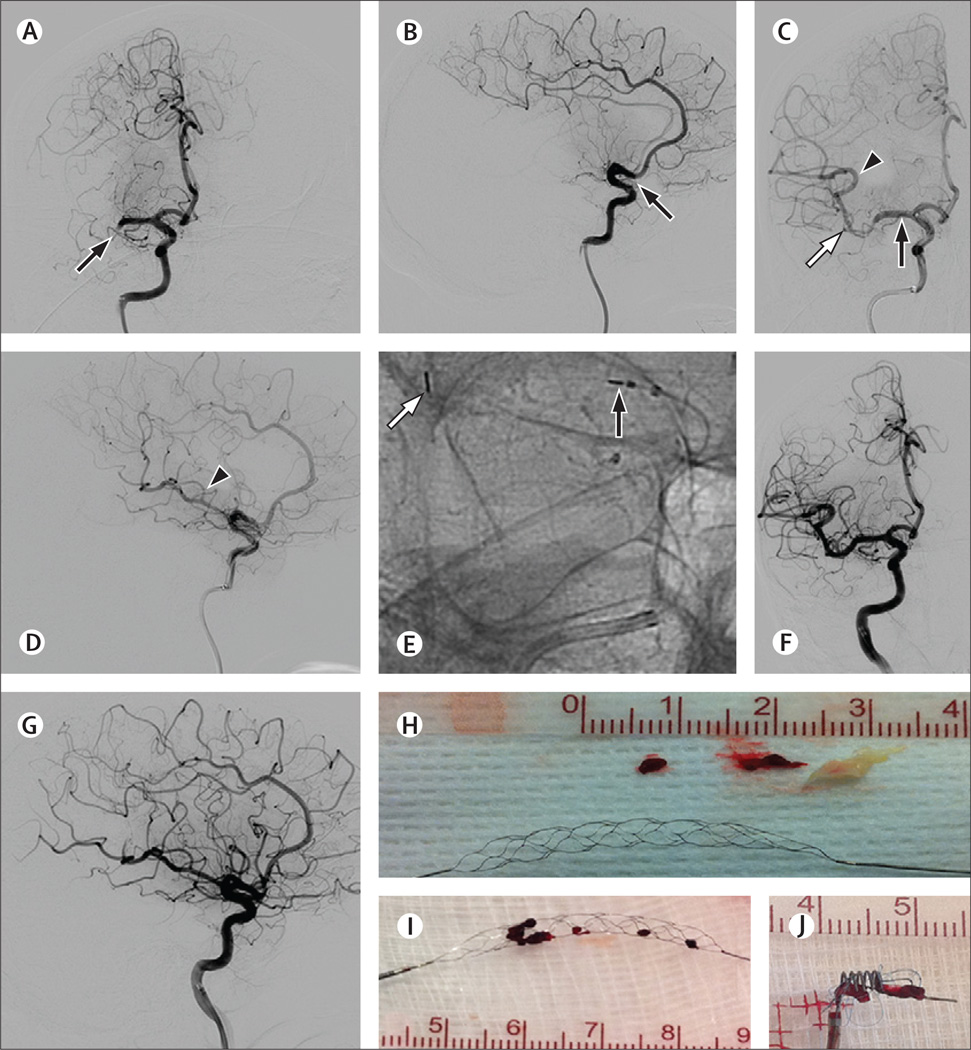
Background: Present mechanical devices are unable to achieve recanalisation in up to 20-40% of large vessel occlusion strokes. We compared efficacy and safety of the Trevo Retriever, a new stent-like device, with its US Food and Drug Administration-cleared predecessor, the Merci Retriever.
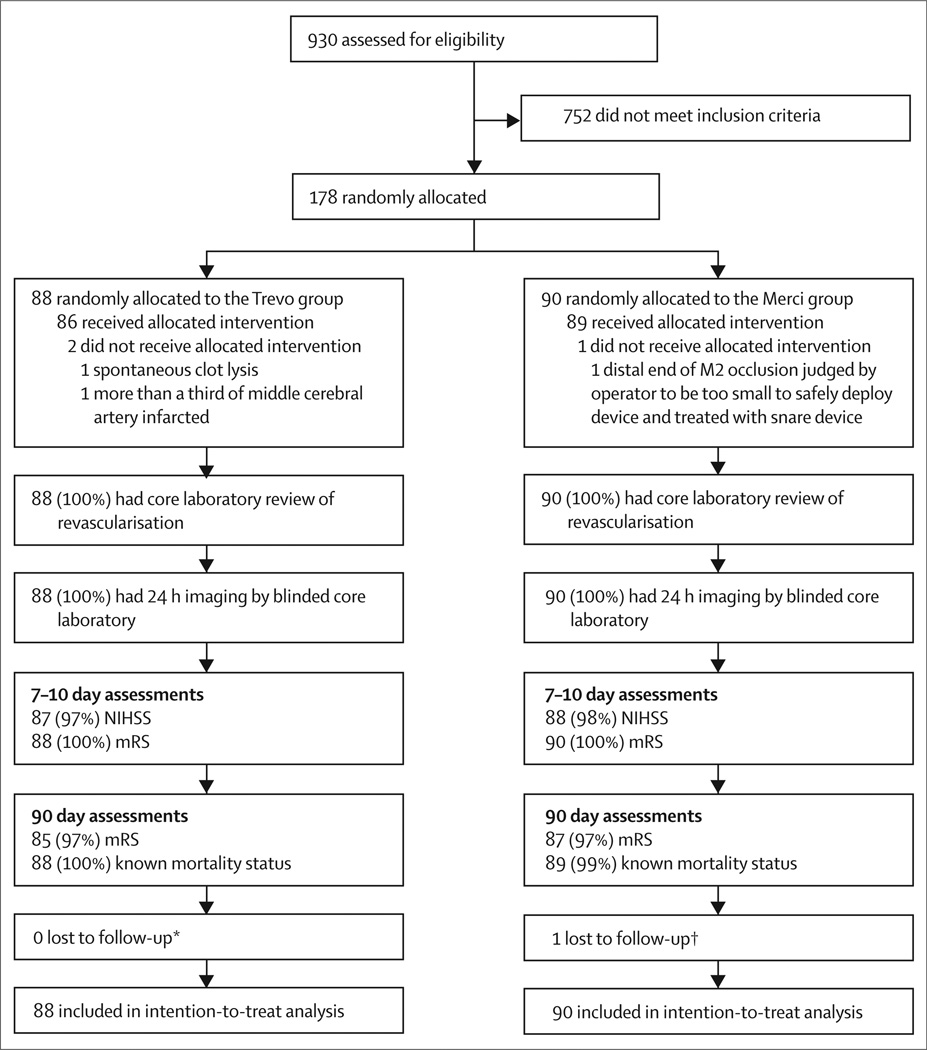
Methods: In this open-label randomised controlled trial, we recruited patients at 26 sites in the USA and one in Spain. We included adults aged 18-85 years with angiographically confirmed large vessel occlusion strokes and US National Institutes of Health Stroke Scale (NIHSS) scores of 8-29 within 8 h of symptom onset. We randomly assigned patients (1:1) with sequentially numbered sealed envelopes to thrombectomy with Trevo or Merci devices. Randomisation was stratified by age (≤68 years vs 69-85 years) and NIHSS scores (≤18 vs 19-29) with alternating blocks of various sizes. The primary efficacy endpoint, assessed by an unmasked core laboratory, was thrombolysis in cerebral infarction (TICI) scores of 2 or greater reperfusion with the assigned device alone. The primary safety endpoint was a composite of procedure-related adverse events. Analyses were done by intention to treat. This study is registered with ClinicalTrials.gov, number NCT01270867.
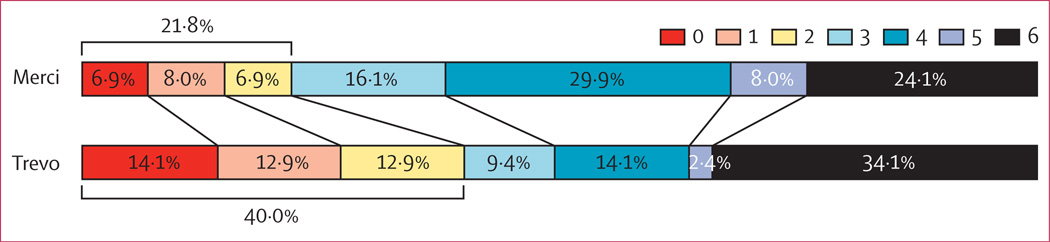
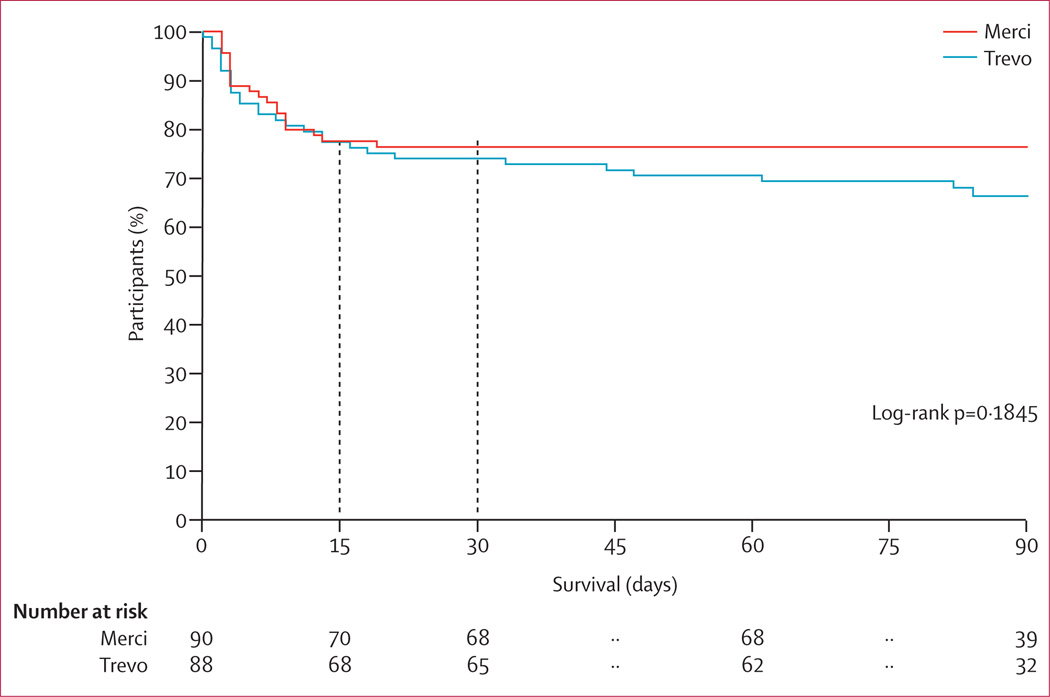
Findings: Between Feb 3, 2011, and Dec 1, 2011, we randomly assigned 88 patients to the Trevo Retriever group and 90 patients to Merci Retriever group. 76 (86%) patients in the Trevo group and 54 (60%) in the Merci group met the primary endpoint after the assigned device was used (odds ratio 4·22, 95% CI 1·92-9·69; p(superiority)<0·0001). Incidence of the primary safety endpoint did not differ between groups (13 [15%] patients in the Trevo group vs 21 [23%] in the Merci group; p=0·1826).
Interpretation: Patients who have had large vessel occlusion strokes but are ineligible for (or refractory to) intravenous tissue plasminogen activator should be treated with the Trevo Retriever in preference to the Merci Retriever.
Funding: Stryker Neurovascular.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
RGN has served on scientific advisory boards for Stryker/Concentric Medical, Covidien/ev3 Neurovascular, CoAxia, Penumbra, Rapid Medical, Reverse Medical, and Neurointervention. HLL has served on scientific advisory boards for Stryker/Concentric Medical and CoAxia. RG has served on scientific advisory boards for Stryker/Concentric Medical, Covidien/ev3 Neurovascular, CoAxia, Rapid Medical, Reverse Medical, and Neurointervention. TGJ has served on scientific advisory boards for Stryker/Concentric Medical, Covidien/ev3 Neurovascular, CoAxia, and Neurointervention. GWA has served on scientific advisory boards for Stryker/Concentric Medical, consulted for Covidien, and has an equity interest in iSchemaView. GAW is an employee of Stryker/Concentric Medical. DSL has served on scientific advisory boards for Stryker/ Concentric Medical, Covidien/ev3 Neurovascular, and CoAxia. WSS has served on scientific advisory boards for Stryker/Concentric Medical.
Figures
Comment in
-
Assessment of stent retrievers in acute ischaemic stroke.Lancet. 2012 Oct 6;380(9849):1208-10. doi: 10.1016/S0140-6736(12)61302-6. Epub 2012 Aug 26. Lancet. 2012. PMID: 22932712 No abstract available.
-
Stroke: New mechanical clot retrieval devices show superiority in patients with acute ischaemic stroke.Nat Rev Neurol. 2012 Oct;8(10):531. doi: 10.1038/nrneurol.2012.196. Epub 2012 Sep 18. Nat Rev Neurol. 2012. PMID: 22986434 No abstract available.
-
[Our new Superman - stent of steel. The hero in metal meshwork].Radiologe. 2013 Jul;53(7):580-1. doi: 10.1007/s00117-013-2518-1. Radiologe. 2013. PMID: 23719754 German. No abstract available.
References
-
- Katzan IL, Hammer MD, Hixson ED, Furlan AJ, Abou-Chebl A, Nadzam DM. Utilization of intravenous tissue plasminogen activator for acute ischemic stroke. Arch Neurol. 2004;61:346–350. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4·5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. - PubMed
-
- Marler JR, Tilley BC, Lu M, et al. Early stroke treatment associated with better outcome: the NINDS rt-PA stroke study. Neurology. 2000;55:1649–1655. - PubMed
-
- Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363:768–774. - PubMed
-
- Bhatia R, Hill MD, Shobha N, et al. Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator in ischemic stroke: real-world experience and a call for action. Stroke. 2010;41:2254–2258. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
