

Ultrasound-guided combined intermediate and deep cervical plexus nerve block for regional anaesthesia in oral and maxillofacial surgery
- PMID: 22933534
- PMCID: PMC3699012
- DOI: 10.1259/dmfr/29945724
Ultrasound-guided combined intermediate and deep cervical plexus nerve block for regional anaesthesia in oral and maxillofacial surgery
Abstract
Objectives: We examined the application of an ultrasound-guided combined intermediate and deep cervical plexus nerve block for regional anaesthesia in patients undergoing oral and maxillofacial surgery.
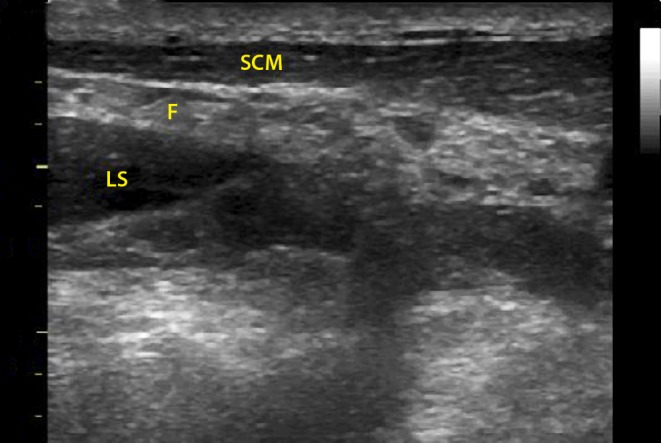
Methods: A total of 19 patients receiving ultrasound-guided combined intermediate and deep cervical plexus anaesthesia followed by neck surgery were examined prospectively. The sternocleidomastoid and the levator of the scapula muscles as well as the cervical transverse processes were used as easily depicted ultrasound landmarks for the injection of local anaesthetics. Under ultrasound guidance, a needle was advanced in the fascial band between the sternocleidomastoid and the levator of the scapula muscles and 15 ml of ropivacaine 0.75% was injected. Afterwards, the needle was advanced between the levator of the scapula and the hyperechoic contour of the cervical transverse processes and a further 15 ml of ropivacaine 0.75% was injected. The sensory block of the cervical nerve plexus, the analgesic efficacy of the block within 24 h after injection and potential block-related complications were assessed.
Results: All patients showed a complete cervical plexus nerve block. No patient required analgesics within the first 24 h after anaesthesia. Two cases of blood aspiration were recorded. No further cervical plexus block-related complications were observed.
Conclusions: Ultrasound-guided combined intermediate and deep cervical plexus block is a feasible, effective and safe method for oral and maxillofacial surgical procedures.
Figures




References
-
- Pandit JJ, Satya-Krishna R, Gration P. Superficial or deep cervical plexus block for carotid endarterectomy: a systematic review of complications. Br J Anaesth 2007; 99: 159–169 - PubMed
-
- Aunac S, Carlier M, Singelyn F, De Kock M. The analgesic efficacy of bilateral combined superficial and deep cervical plexus block administered before thyroid surgery under general anesthesia. Anesth Analg 2002; 95: 746–750 - PubMed
-
- Pintaric TS, Hocevar M, Jereb S, Casati A, Jankovic VN. A prospective, randomized comparison between combined (deep and superficial) and superficial cervical plexus block with levobupivacaine for minimally invasive parathyroidectomy. Anesth Analg 2007; 105: 1160–1163 - PubMed
-
- Suresh S, Templeton L. Superficial cervical plexus block for vocal cord surgery in an awake pediatric patient. Anesth Analg 2004; 98: 1656–1657 - PubMed
-
- Usui Y, Kobayashi T, Kakinuma H, Watanabe K, Kitajima T, Matsuno K. An anatomical basis for blocking of the deep cervical plexus and cervical sympathetic tract using an ultrasound-guided technique. Anesth Analg 2010; 110: 964–968 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
