

Role of radiotherapy in melanoma management
- PMID: 22933884
- PMCID: PMC3423668
- DOI: 10.2478/v10019-010-0008-x
Role of radiotherapy in melanoma management
Abstract
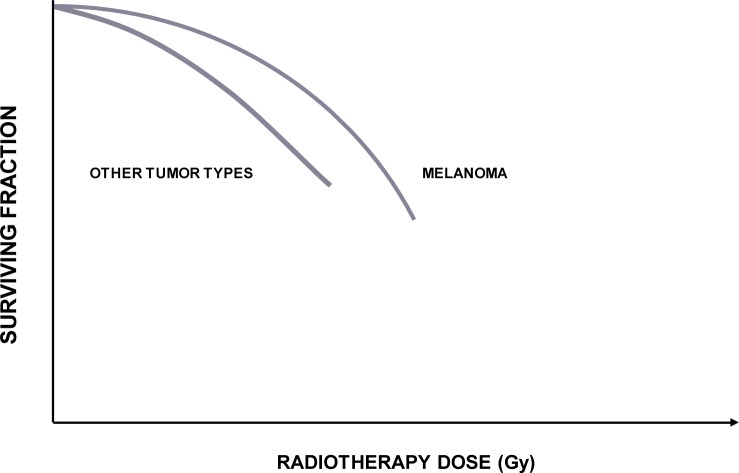
Background: In melanoma, radiotherapy has generally been considered as a palliative treatment option indicated only for advanced cases or disseminated disease. In the 70s of the previous century, the technological advances in radiotherapy, linked to rapid development of computer sciences, resulted in restored interest for radiotherapy in melanoma management. Although a fundamental lack of well designed prospective and/or randomized clinical trials critically influenced the integration of radiotherapy into treatment strategies in melanoma, radiotherapy was recently recognized as an indispensable part in the multidisciplinary management of patients with melanoma. Altogether, approximately 23% of melanoma patients should receive at least one course of radiotherapy during the course of the disease. In this review, radiobiological properties of melanoma that govern the decisions for the fractionation patterns used in the treatment of this disease are described. Moreover, the indications for irradiation and the results of pertinent clinical studies from the literature, creating a rationale for the use of radiotherapy in the management of this disease, are reviewed and a brief description of radiotherapy techniques is given.
Conclusions: Basic treatment modality in melanoma is surgery. However, whenever surgery is not radical or there are adverse prognostic factors identified on histopathological examination of resected tissue specimen, it needs to be supplemented. Also, in patients with unresectable disease or in those not being suitable for major surgery or who refuse proposed surgical intervention, other effective mode(s) of therapy need to be implemented. From this perspective, supported by clinical experiences and literature results, radiotherapy is a valuable option: it is effective and safe, in curative and palliative setting.
Keywords: fractionation; indications; melanoma; radiobiology; radiotherapy; toxicity.
Figures
References
-
- de Vries E, Bray FI, Coebergh JW, Parkin DM. Changing epidemiology of malignant cutaneous melanoma in Europe 1953–1997: rising trends in incidence and mortality but recent stabilization in western Europe and decreases in Scandinavia. Int J Cancer. 2003;107:119–26. - PubMed
-
- Cancer incidence in Slovenia 1997. Report no. 39. Ljubljana: Institute of Oncology Ljubljana, Cancer Registry of Republic of Slovenia; 2000.
-
- Cancer incidence in Slovenia 2006. Report no. 48. Ljubljana: Institute of Oncology Ljubljana, Cancer Registry of Republic of Slovenia; 2009.
-
- Kingham TP, Karakousis G, Ariyan C. Randomized clinical trials in melanoma. Surg Oncol Clin N Am. 2010;19:13–31. - PubMed
-
- Paterson R. Classification of tumours in relation to radiosensitivity. Br J Radiol. 1933;6:218–33.
LinkOut - more resources
Full Text Sources
Other Literature Sources