

Balancing selected medication costs with total number of daily injections: a preference analysis of GnRH-agonist and antagonist protocols by IVF patients
- PMID: 22935199
- PMCID: PMC3447708
- DOI: 10.1186/1477-7827-10-67
Balancing selected medication costs with total number of daily injections: a preference analysis of GnRH-agonist and antagonist protocols by IVF patients
Abstract
Background: During in vitro fertilization (IVF), fertility patients are expected to self-administer many injections as part of this treatment. While newer medications have been developed to substantially reduce the number of these injections, such agents are typically much more expensive. Considering these differences in both cost and number of injections, this study compared patient preferences between GnRH-agonist and GnRH-antagonist based protocols in IVF.
Methods: Data were collected by voluntary, anonymous questionnaire at first consultation appointment. Patient opinion concerning total number of s.c. injections as a function of non-reimbursed patient cost associated with GnRH-agonist [A] and GnRH-antagonist [B] protocols in IVF was studied.
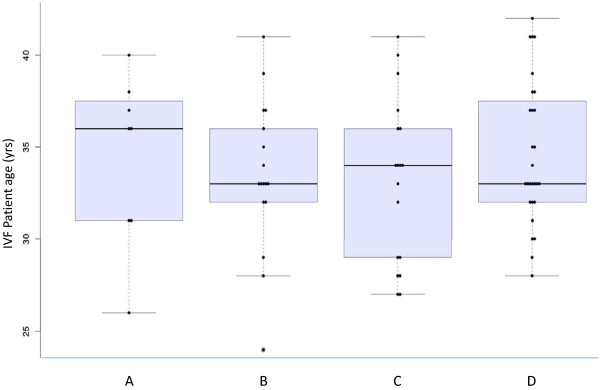
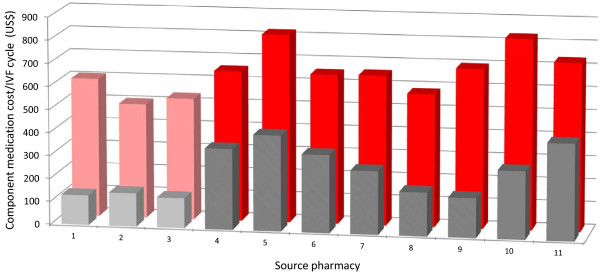
Results: Completed questionnaires (n = 71) revealed a mean +/- SD patient age of 34 +/- 4.1 yrs. Most (83.1%) had no prior IVF experience; 2.8% reported another medical condition requiring self-administration of subcutaneous medication(s). When out-of-pocket cost for [A] and [B] were identical, preference for [B] was registered by 50.7% patients. The tendency to favor protocol [B] was weaker among patients with a health occupation. Estimated patient costs for [A] and [B] were $259.82 +/- 11.75 and $654.55 +/- 106.34, respectively (p < 0.005). Measured patient preference for [B] diminished as the cost difference increased.
Conclusions: This investigation found consistently higher non-reimbursed direct medication costs for GnRH-antagonist IVF vs. GnRH-agonist IVF protocols. A conditional preference to minimize downregulation (using GnRH-antagonist) was noted among some, but not all, IVF patient sub-groups. Compared to IVF patients with a health occupation, the preference for GnRH-antagonist was weaker than for other patients. While reducing total number of injections by using GnRH-antagonist is a desirable goal, it appears this advantage is not perceived equally by all IVF patients and its utility is likely discounted heavily by patients when nonreimbursed medication costs reach a critical level.
Figures
References
-
- Ekerhovd E. Use of GnRH antagonist for in vitro fertilization. Tidsskr Nor Laegeforen. 2011;131:1649–1652. - PubMed
-
- Kdous M, Chaker A, Bouyahia M, Zhioua F, Zhioua A. Increased risk of early pregnancy loss and lower live birth rate with GNRH antagonist vs. long GNRH agonist protocol in PCOS women undergoing controlled ovarian hyperstimulation. Tunis Med. 2009;87:834–842. - PubMed
-
- Lainas TG, Sfontouris IA, Zorzovilis IZ, Petsas GK, Lainas GT, Alexopoulou E, Kolibianakis EM. Flexible GnRH antagonist protocol versus GnRH agonist long protocol in patients with polycystic ovary syndrome treated for IVF: a prospective randomised controlled trial (RCT) Hum Reprod. 2010;25:683–689. doi: 10.1093/humrep/dep436. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
