

Assessment of intramyocardial hemorrhage by T1-weighted cardiovascular magnetic resonance in reperfused acute myocardial infarction
- PMID: 22935462
- PMCID: PMC3457904
- DOI: 10.1186/1532-429X-14-59
Assessment of intramyocardial hemorrhage by T1-weighted cardiovascular magnetic resonance in reperfused acute myocardial infarction
Abstract
Background: Intramyocardialhemorrhage (IMH) reflects severe reperfusion injury in acute myocardial infarction. Non-invasive detection of IMH by cardiovascular magnetic resonance (CMR) may serve as a surrogate marker to evaluate the effect of preventive measures to reduce reperfusion injury and hence provide additional prognostic information. We sought to investigate whether IMH could be detected by CMR exploiting the T1 shortening effect of methemoglobin in an experimental model of acute myocardial infarction. The results were compared to T2-weighthed short tau inversion recovery (T2-STIR), and T2*-weighted(T2*W) sequences.
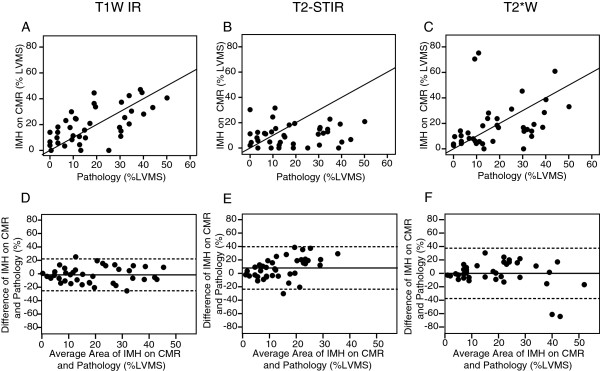
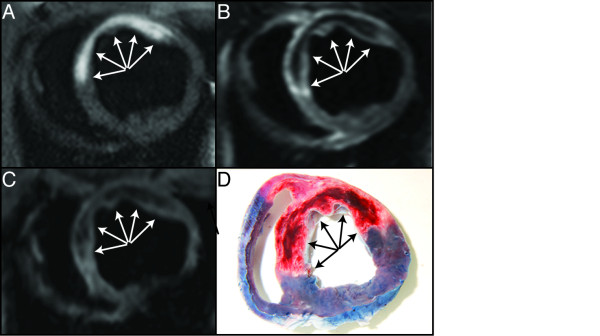
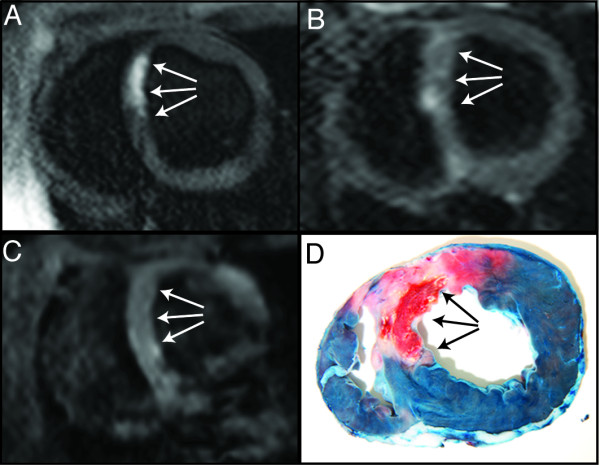
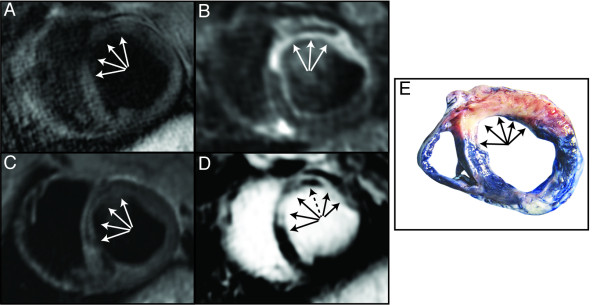
Methods and results: IMH was induced in ten 40 kg pigs by 50-min balloon occlusion of the mid LAD followed by reperfusion. Between 4-9 days (average 4.8) post-injury, the left ventricular myocardium was assessed by T1-weigthed Inversion Recovery(T1W-IR), T2-STIR, and T2*W sequences. All CMR images were matched to histopathology and compared with the area of IMH. The difference between the size of the IMH area detected on T1W-IR images and pathology was -1.6 ± 11.3% (limits of agreement, -24%-21%), for the T2*W images the difference was -0.1 ± 18.3% (limits of agreement, -36.8%-36.6%), and for T2-STIR the difference was 8.0 ± 15.5% (limits of agreement, -23%-39%). By T1W IR the diagnostic sensitivity of IMH was 90% and specificity 70%, for T2*W imaging the sensitivity was 70% and specificity 50%, and for T2-STIR sensitivity for imaging IMH was 50% and specificity 60%.
Conclusion: T1-weigthed non-contrast enhanced CMR detects IMH with high sensitivity and specificity and may become a diagnostic tool for detection of IMH in patients with myocardial infarction.
Figures
Similar articles
-
Susceptibility-weighted cardiovascular magnetic resonance in comparison to T2 and T2 star imaging for detection of intramyocardial hemorrhage following acute myocardial infarction at 3 Tesla.J Cardiovasc Magn Reson. 2014 Oct 28;16(1):86. doi: 10.1186/s12968-014-0086-9. J Cardiovasc Magn Reson. 2014. PMID: 25356834 Free PMC article.
-
The relation between hypointense core, microvascular obstruction and intramyocardial haemorrhage in acute reperfused myocardial infarction assessed by cardiac magnetic resonance imaging.Eur Radiol. 2014 Dec;24(12):3277-88. doi: 10.1007/s00330-014-3318-3. Epub 2014 Aug 6. Eur Radiol. 2014. PMID: 25097126 Free PMC article.
-
Head-to-head comparison of multiple cardiovascular magnetic resonance techniques for the detection and quantification of intramyocardial haemorrhage in patients with ST-elevation myocardial infarction.Eur Radiol. 2021 Mar;31(3):1245-1256. doi: 10.1007/s00330-020-07254-1. Epub 2020 Sep 14. Eur Radiol. 2021. PMID: 32929640 Free PMC article.
-
Cardiovascular MR T2-STIR imaging does not discriminate between intramyocardial haemorrhage and microvascular obstruction during the subacute phase of a reperfused myocardial infarction.Open Heart. 2016 Apr 20;3(1):e000346. doi: 10.1136/openhrt-2015-000346. eCollection 2016. Open Heart. 2016. PMID: 27110375 Free PMC article.
-
T2-weighted cardiovascular magnetic resonance in acute cardiac disease.J Cardiovasc Magn Reson. 2011 Feb 18;13(1):13. doi: 10.1186/1532-429X-13-13. J Cardiovasc Magn Reson. 2011. PMID: 21332972 Free PMC article. Review.
Cited by
-
Determination of location, size, and transmurality of chronic myocardial infarction without exogenous contrast media by using cardiac magnetic resonance imaging at 3 T.Circ Cardiovasc Imaging. 2014 May;7(3):471-81. doi: 10.1161/CIRCIMAGING.113.001541. Epub 2014 Mar 28. Circ Cardiovasc Imaging. 2014. PMID: 24682268 Free PMC article.
-
Review of Journal of Cardiovascular Magnetic Resonance 2012.J Cardiovasc Magn Reson. 2013 Sep 4;15(1):76. doi: 10.1186/1532-429X-15-76. J Cardiovasc Magn Reson. 2013. PMID: 24006874 Free PMC article. Review.
-
Multiparametric CMR imaging of infarct remodeling in a percutaneous reperfused Yucatan mini-pig model.NMR Biomed. 2017 May;30(5):10.1002/nbm.3693. doi: 10.1002/nbm.3693. Epub 2017 Feb 6. NMR Biomed. 2017. PMID: 28164391 Free PMC article.
-
Tissue Characterization in Cardiology: Moving Beyond Function.Adv Exp Med Biol. 2021;1337:89-97. doi: 10.1007/978-3-030-78771-4_11. Adv Exp Med Biol. 2021. PMID: 34972895
-
A Case of Low T1 Mapping Values in Myocardial Calcifications in a Patient With End-Stage Renal Disease.Cureus. 2025 Apr 17;17(4):e82431. doi: 10.7759/cureus.82431. eCollection 2025 Apr. Cureus. 2025. PMID: 40385786 Free PMC article.
References
-
- Grines CL, Browne KF, Marco J, Rothbaum D, Stone GW, O'Keefe J, Overlie P, Donohue B, Chelliah N, Timmis GC. A comparison of immediate angioplasty with thrombolytic therapy for acute myocardial infarction. The primary angioplasty in myocardial infarction study group. N Engl J Med. 1993;328:673–679. doi: 10.1056/NEJM199303113281001. - DOI - PubMed
-
- Asanuma T, Tanabe K, Ochiai K, Yoshitomi H, Nakamura K, Murakami Y, Sano K, Shimada T, Murakami R, Morioka S, Beppu S. Relationship between progressive microvascular damage and intramyocardial hemorrhage in patients with reperfused anterior myocardial infarction: myocardial contrast echocardiographic study. Circulation. 1997;96:448–453. doi: 10.1161/01.CIR.96.2.448. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
