

Association of systolic and diastolic blood pressure and all cause mortality in people with newly diagnosed type 2 diabetes: retrospective cohort study
- PMID: 22936794
- PMCID: PMC3431284
- DOI: 10.1136/bmj.e5567
Association of systolic and diastolic blood pressure and all cause mortality in people with newly diagnosed type 2 diabetes: retrospective cohort study
Abstract
Objective: To examine the effect of systolic and diastolic blood pressure achieved in the first year of treatment on all cause mortality in patients newly diagnosed with type 2 diabetes, with and without established cardiovascular disease.
Design: Retrospective cohort study.
Setting: United Kingdom General Practice Research Database, between 1990 and 2005.
Participants: 126,092 adult patients (age ≥ 18 years) with a new diagnosis of type 2 diabetes who had been registered with participating practices for at least 12 months.
Main outcome measure: All cause mortality.
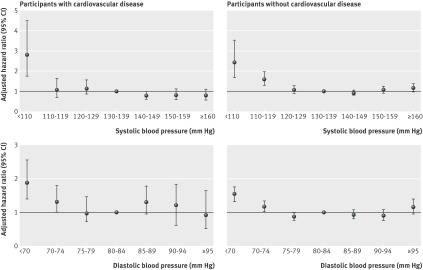
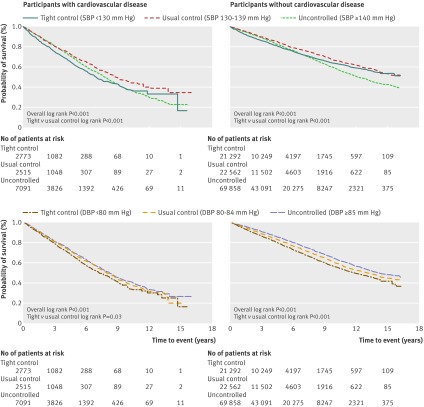
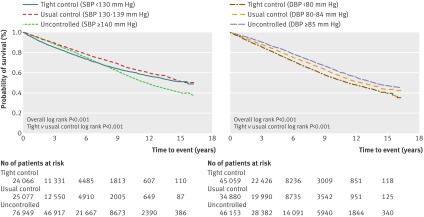
Results: Before diagnosis, 12,379 (9.8%) patients had established cardiovascular disease (myocardial infarction or stroke). During a median follow-up of 3.5 years, we recorded 25,495 (20.2%) deaths. In people with cardiovascular disease, tight control of systolic (<130 mm Hg) and diastolic (<80 mm Hg) blood pressure was not associated with improved survival, after adjustment for baseline characteristics (age at diagnosis, sex, practice level clustering, deprivation score, body mass index, smoking, HbA(1c) and cholesterol levels, and blood pressure). Low blood pressure was also associated with an increased risk of all cause mortality. Compared with patients who received usual control of systolic blood pressure (130-139 mm Hg), the hazard ratio of all cause mortality was 2.79 (95% confidence interval 1.74 to 4.48, P<0.001) for systolic blood pressure at 110 mm Hg. Compared with patients who received usual control of diastolic blood pressure (80-84 mm Hg), the hazard ratios were 1.32 (1.02 to 1.78, P=0.04) and 1.89 (1.40 to 2.56, P<0.001) for diastolic blood pressures at 70-74 mm Hg and lower than 70 mm Hg, respectively. Similar associations were found in people without cardiovascular disease. Subgroup analyses of people diagnosed with hypertension and who received treatment for hypertension confirmed initial findings.
Conclusion: Blood pressure below 130/80 mm Hg was not associated with reduced risk of all cause mortality in patients with newly diagnosed diabetes, with or without known cardiovascular disease. Low blood pressure, particularly below 110/75 mm Hg, was associated with an increased risk for poor outcomes.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Lower blood pressure associated with higher mortality in retrospective study of patients with newly diagnosed type 2 diabetes.Evid Based Med. 2013 Aug;18(4):e35. doi: 10.1136/eb-2012-101060. Epub 2012 Nov 20. Evid Based Med. 2013. PMID: 23173154 No abstract available.
-
[Type 2 diabetes: low blood pressure increases risk of mortality].Dtsch Med Wochenschr. 2012 Oct;137(42):2135. doi: 10.1055/s-0032-1328974. Dtsch Med Wochenschr. 2012. PMID: 23227520 German. No abstract available.
References
-
- Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al. 2007 Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2007;25:1105-87. - PubMed
-
- Zanchetti A, Grassi G, Mancia G. When should antihypertensive drug treatment be initiated and to what levels should systolic blood pressure be lowered? A critical reappraisal. J Hypertens 2009;27:923-34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous