

Long-term sensory stimulation therapy improves hand function and restores cortical responsiveness in patients with chronic cerebral lesions. Three single case studies
- PMID: 22936907
- PMCID: PMC3427543
- DOI: 10.3389/fnhum.2012.00244
Long-term sensory stimulation therapy improves hand function and restores cortical responsiveness in patients with chronic cerebral lesions. Three single case studies
Abstract
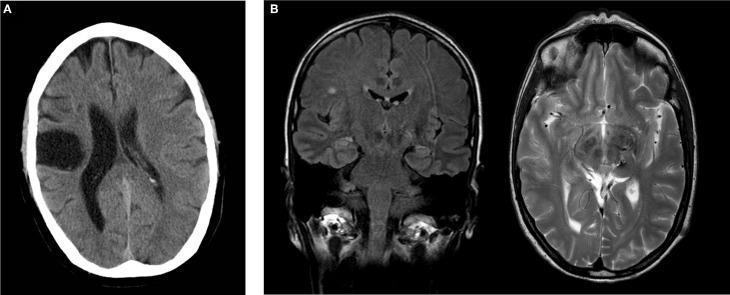
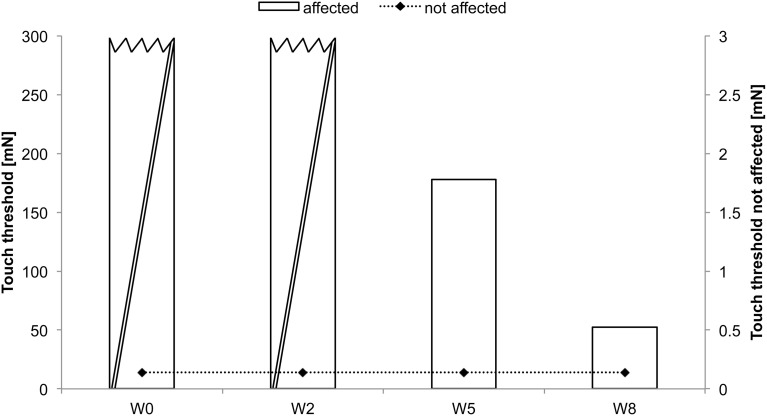
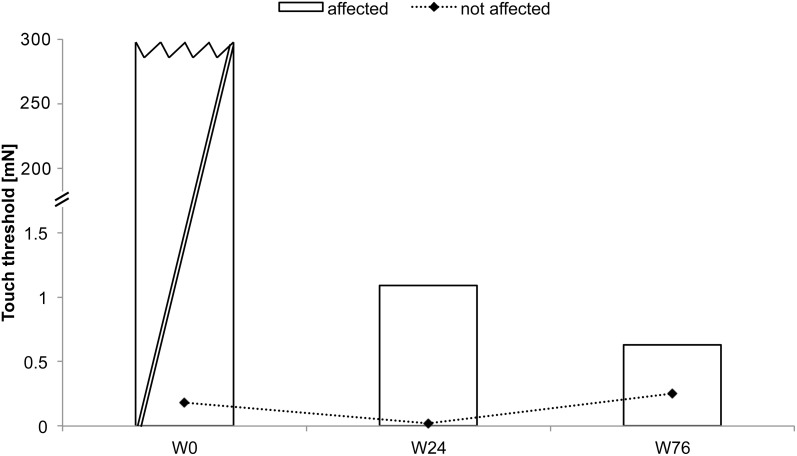
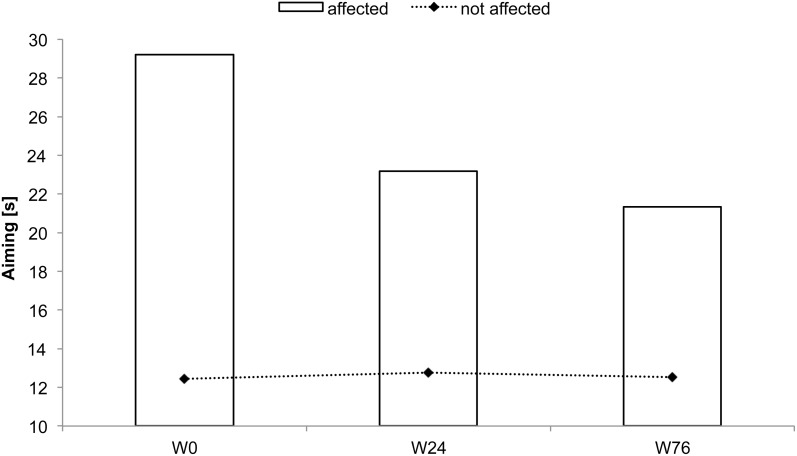
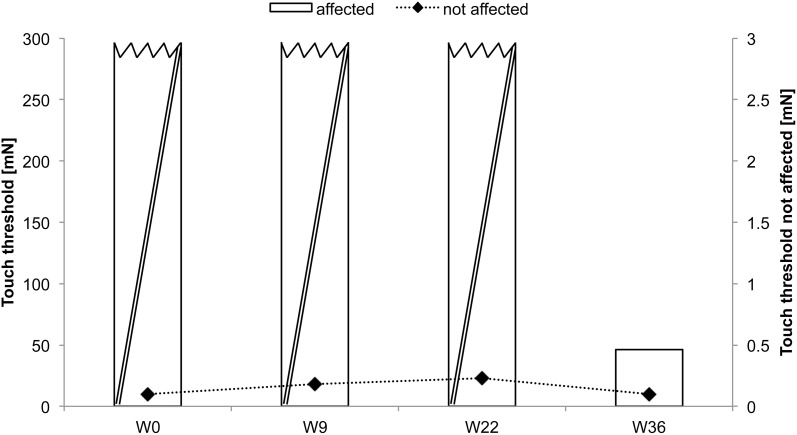
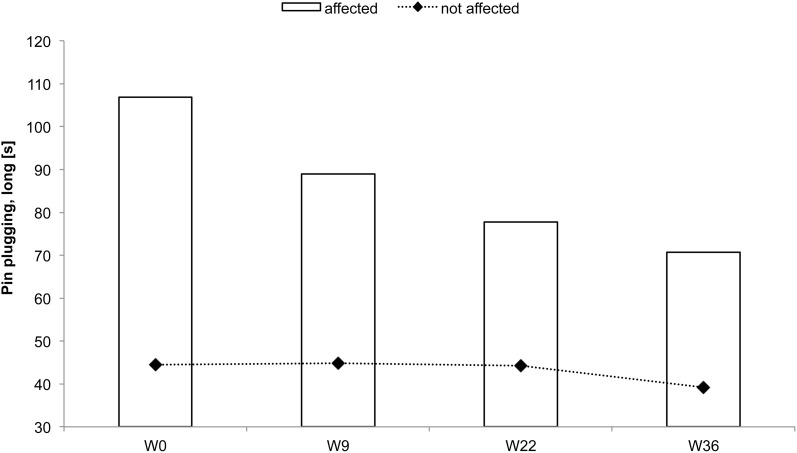
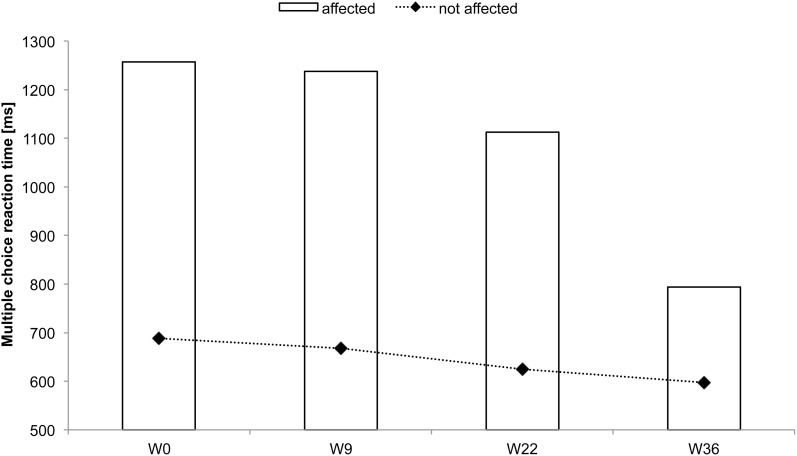
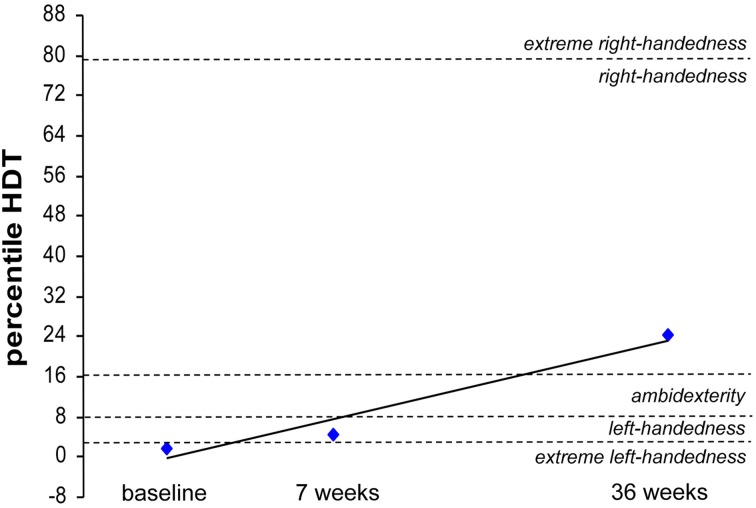
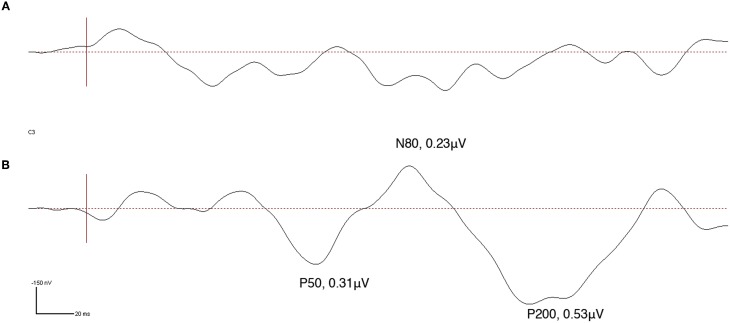
Rehabilitation of sensorimotor impairment resulting from cerebral lesion (CL) utilizes task specific training and massed practice to drive reorganization and sensorimotor improvement due to induction of neuroplasticity mechanisms. Loss of sensory abilities often complicates recovery, and thus the individual's ability to use the affected body part for functional tasks. Therefore, the development of additional and alternative approaches that supplement, enhance, or even replace conventional training procedures would be advantageous. Repetitive sensory stimulation protocols (rSS) have been shown to evoke sensorimotor improvements of the affected limb in patients with chronic stroke. However, the possible impact of long-term rSS on sensorimotor performance of patients with CL, where the incident dated back many years remains unclear. The particular advantage of rSS is its passive nature, which does not require active participation of the subjects. Therefore, rSS can be applied in parallel to other occupations, making the intervention easier to implement and more acceptable to the individual. Here we report the effects of applying rSS for 8, 36, and 76 weeks to the paretic hand of three long-term patients with different types of CL. Different behavioral tests were used to assess sensory and/or sensorimotor performance of the upper extremities prior, after, and during the intervention. In one patient, the impact of long-term rSS on restoration of cortical activation was investigated by recording somatosensory evoked potentials (SEP). After long-term rSS all three patients showed considerable improvements of their sensory and motor abilities. In addition, almost normal evoked potentials could be recorded after rSS in one patient. Our data show that long-term rSS applied to patients with chronic CL can improve tactile and sensorimotor functions, which, however, developed in some cases only after many weeks of stimulation, and continued to further improve on a time scale of months.
Keywords: chronic cerebral lesion; repetitive sensory stimulation; sensorimotor hand function; single case.
Figures
Similar articles
-
Daily repetitive sensory stimulation of the paretic hand for the treatment of sensorimotor deficits in patients with subacute stroke: RESET, a randomized, sham-controlled trial.BMC Neurol. 2018 Jan 9;18(1):2. doi: 10.1186/s12883-017-1006-z. BMC Neurol. 2018. PMID: 29316895 Free PMC article. Clinical Trial.
-
Repetitive tactile stimulation changes resting-state functional connectivity-implications for treatment of sensorimotor decline.Front Hum Neurosci. 2012 May 23;6:144. doi: 10.3389/fnhum.2012.00144. eCollection 2012. Front Hum Neurosci. 2012. PMID: 22654748 Free PMC article.
-
High-Frequency Repetitive Sensory Stimulation as Intervention to Improve Sensory Loss in Patients with Complex Regional Pain Syndrome I.Front Neurol. 2015 Nov 17;6:242. doi: 10.3389/fneur.2015.00242. eCollection 2015. Front Neurol. 2015. PMID: 26635719 Free PMC article.
-
Integrated technology for evaluation of brain function and neural plasticity.Phys Med Rehabil Clin N Am. 2004 Feb;15(1):263-306. doi: 10.1016/s1047-9651(03)00124-4. Phys Med Rehabil Clin N Am. 2004. PMID: 15029909 Review.
-
Does Sensory Retraining Improve Sensation and Sensorimotor Function Following Stroke: A Systematic Review and Meta-Analysis.Front Neurosci. 2019 Apr 30;13:402. doi: 10.3389/fnins.2019.00402. eCollection 2019. Front Neurosci. 2019. PMID: 31114472 Free PMC article.
Cited by
-
Modification of the ladder rung walking task-new options for analysis of skilled movements.Stroke Res Treat. 2013;2013:418627. doi: 10.1155/2013/418627. Epub 2013 Mar 12. Stroke Res Treat. 2013. PMID: 23577278 Free PMC article.
-
Hyperbaric oxygen induces late neuroplasticity in post stroke patients--randomized, prospective trial.PLoS One. 2013;8(1):e53716. doi: 10.1371/journal.pone.0053716. Epub 2013 Jan 15. PLoS One. 2013. PMID: 23335971 Free PMC article. Clinical Trial.
-
Effect of whole-hand water flow stimulation on the neural balance between excitation and inhibition in the primary somatosensory cortex.Front Hum Neurosci. 2022 Oct 25;16:962936. doi: 10.3389/fnhum.2022.962936. eCollection 2022. Front Hum Neurosci. 2022. PMID: 36393986 Free PMC article.
-
Weak but Critical Links between Primary Somatosensory Centers and Motor Cortex during Movement.Front Hum Neurosci. 2018 Jan 17;12:1. doi: 10.3389/fnhum.2018.00001. eCollection 2018. Front Hum Neurosci. 2018. PMID: 29387003 Free PMC article.
-
Reduction of pain sensitivity after somatosensory therapy in adults with cerebral palsy.Front Hum Neurosci. 2013 Jun 24;7:276. doi: 10.3389/fnhum.2013.00276. eCollection 2013. Front Hum Neurosci. 2013. PMID: 23805086 Free PMC article.
References
-
- Alegria J., Bertelson P. (1970). Time uncertainty, number of alternatives and particular signal-response pair as determinantof choice reaction time. Acta Psychol. 33, 36–44
-
- Brown C. E., Aminoltejari K., Erb H., Winship I. R., Murphy T. H. (2009). In vivo voltage-sensitive dye imaging in adult mice reveals that somatosensory maps lost to stroke are replaced over weeks by new structural and functional circuits with prolonged modes of activation within both the peri-infarct zone and distant sites. J. Neurosci. 29, 1719–1734 10.1523/JNEUROSCI.4249-08.2009 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources