

Comparison and temporal trends of three groups with cryptococcosis: HIV-infected, solid organ transplant, and HIV-negative/non-transplant
- PMID: 22937064
- PMCID: PMC3427358
- DOI: 10.1371/journal.pone.0043582
Comparison and temporal trends of three groups with cryptococcosis: HIV-infected, solid organ transplant, and HIV-negative/non-transplant
Erratum in
- PLoS One. 2012;7(10). doi: 10.1371/annotation/a94bc542-6682-4579-a315-57019cef7e0e doi: 10.1371/annotation/a94bc542-6682-4579-a315-57019cef7e0e
Abstract
Background: The Infectious Disease Society of America (IDSA) 2010 Clinical Practice Guidelines for the management of cryptococcosis outlined three key populations at risk of disease: (1) HIV-infected, (2) transplant recipient, and (3) HIV-negative/non-transplant. However, direct comparisons of management, severity and outcomes of these groups have not been conducted.
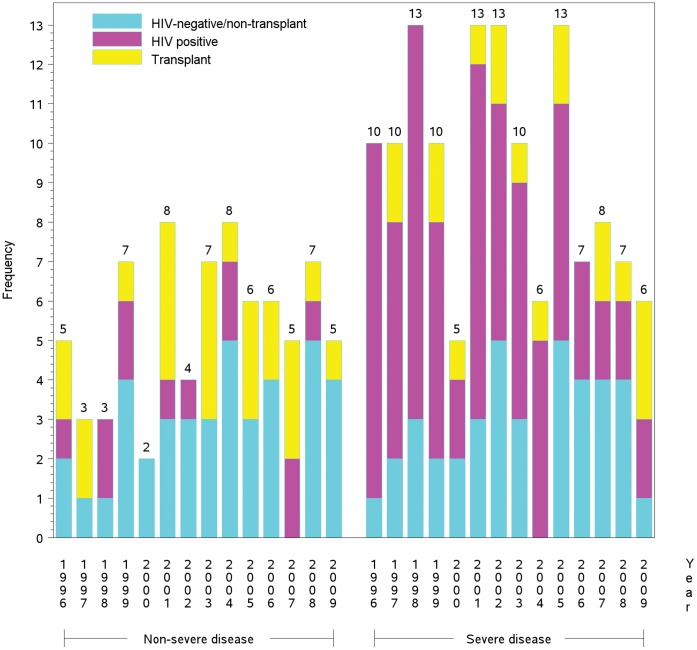
Methodology/principal findings: Annual changes in frequency of cryptococcosis diagnoses, cryptococcosis-attributable mortality and mortality were captured. Differences examined between severe and non-severe disease within the context of the three groups included: demographics, symptoms, microbiology, clinical management and treatment. An average of nearly 15 patients per year presented at Duke University Medical Center (DUMC) with cryptococcosis. Out of 207 study patients, 86 (42%) were HIV-positive, 42 (20%) were transplant recipients, and 79 (38%) were HIV-negative/non-transplant. HIV-infected individuals had profound CD4 lymphocytopenia and a majority had elevated intracranial pressure. Transplant recipients commonly (38%) had renal dysfunction. Nearly one-quarter (24%) had their immunosuppressive regimens stopped or changed. The HIV-negative/non-transplant population reported longer duration of symptoms than HIV-positive or transplant recipients and 28% (22/79) had liver insufficiency or underlying hematological malignancies. HIV-positive and HIV-negative/non-transplant patients accounted for 89% of severe disease cryptococcosis-attributable deaths and 86% of all-cause mortality.
Conclusions/significance: In this single-center study, the frequency of cryptococcosis did not change in the last two decades, although the underlying case mix shifted (fewer HIV-positive cases, stable transplant cases, more cases with neither). Cryptococcosis had a relatively uniform and informed treatment strategy, but disease-attributable mortality was still common.
Conflict of interest statement
Figures
References
-
- Casadevall A, Perfect JR (1998) Cryptococcus neoformans. Washington, D.C.: ASM Press. viii, 541 p.
-
- Palella Jr FJ, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, et al. (1998) Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 338: 853–860. - PubMed
-
- Rust DM, Jameson G (1998) The novel lipid delivery system of amphotericin B: drug profile and relevance to clinical practice. Oncol Nurs Forum 25: 35–48. - PubMed
-
- Saag MS, Graybill RJ, Larsen RA, Pappas PG, Perfect JR, et al. (2000) Practice guidelines for the management of cryptococcal disease. Infectious Diseases Society of America. Clin Infect Dis 30: 710–718. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
