

Glioblastoma presenting with steroid-induced pseudoregression of contrast enhancement on magnetic resonance imaging
- PMID: 22937360
- PMCID: PMC3420373
- DOI: 10.1155/2012/816873
Glioblastoma presenting with steroid-induced pseudoregression of contrast enhancement on magnetic resonance imaging
Abstract
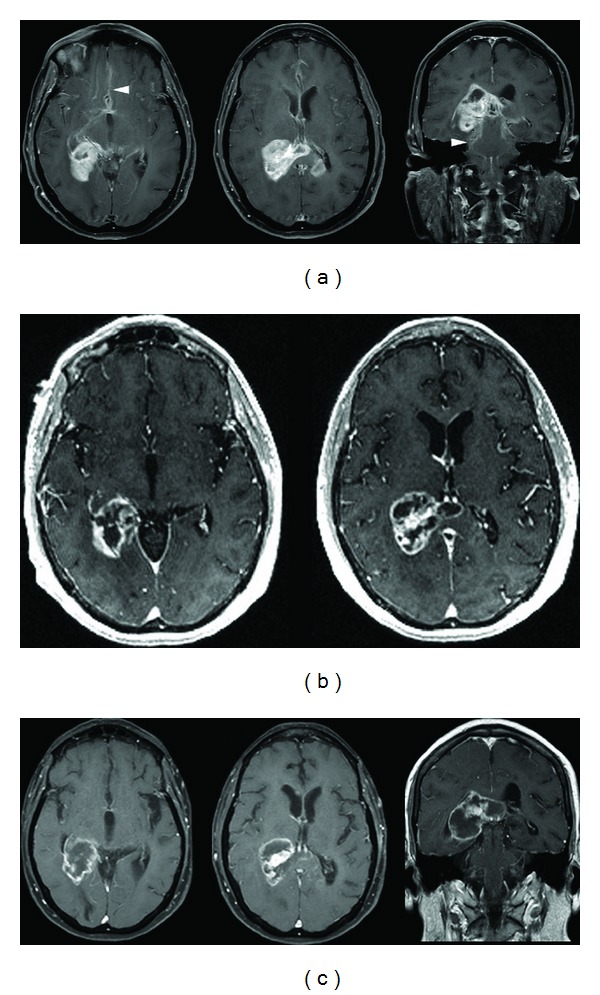
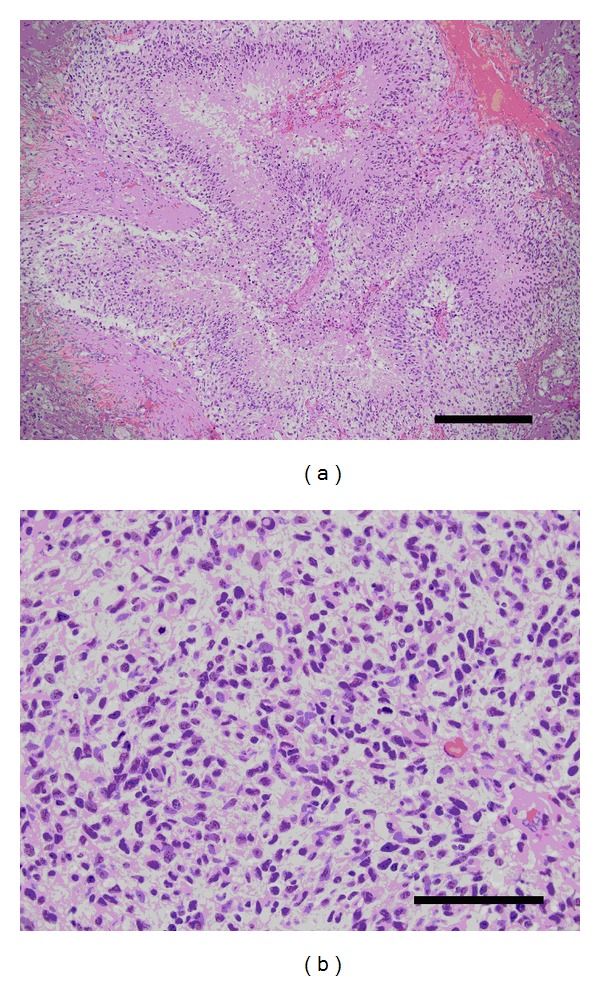
Corticosteroid-induced reduction in contrast enhancement on radiographic imaging is most commonly associated with lymphoma but has been reported in other entities, including glioma. This finding may represent a diagnostic dilemma. Concern that steroid-induced cytotoxicity obscures histological diagnosis of suspected lymphoma may lead to postponement of a biopsy. If glioma is not considered in the differential diagnosis, reduction in tumor contrast enhancement may be misinterpreted as disease regression rather than a transient radiographic change. We report a case of a patient with an enhancing right temporoparietal mass adjacent to the atrium of the lateral ventricle. After treatment with dexamethasone was started, the mass exhibited marked reduction in contrast enhancement, with symptom improvement. The clinical course suggested lymphoma, and surgery was not performed. Subsequent screening for extra-axial lymphoma was negative. Two weeks later, the patient developed worsening symptoms, and repeat T1-weighted imaging showed interval increase in size and enhancement. The findings suggested a possible diagnosis of malignant glioma. The patient underwent a stereotactic-guided craniotomy for excision of the right temporoparietal mass lesion. Final histological diagnosis was glioblastoma multiforme, World Health Organization grade IV.
Figures
References
-
- Bromberg JEC, Siemers MD, Taphoorn MJB. Is a “vanishing tumor” always a lymphoma? Neurology. 2002;59(5):762–764. - PubMed
-
- Cairncross JG, Macdonald DR, Pexman JHW, Ives FJ. Steroid-induced CT changes in patients with recurrent malignant glioma. Neurology. 1988;38(5):724–726. - PubMed
-
- Goh JJ, See SJ, Ang E, Ng WH. Vanishing glioblastoma after corticosteroid therapy. Journal of Clinical Neuroscience. 2009;16(9):1226–1228. - PubMed
-
- Hasegawa H, Pal D, Ramirez R, Ismail A, Marks P. Glioblastoma multiforme fades on CT imaging after dexamethasone therapy. Journal of Clinical Neuroscience. 2009;16(12):1707–1708. - PubMed
LinkOut - more resources
Full Text Sources
