

Outpatient management of severe early OHSS by administration of GnRH antagonist in the luteal phase: an observational cohort study
- PMID: 22938051
- PMCID: PMC3489837
- DOI: 10.1186/1477-7827-10-69
Outpatient management of severe early OHSS by administration of GnRH antagonist in the luteal phase: an observational cohort study
Abstract
Background: Management of established severe OHSS requires prolonged hospitalization, occasionally in intensive care units, accompanied by multiple ascites punctures, correction of intravascular fluid volume and electrolyte imbalance. The aim of the present study was to evaluate whether it is feasible to manage women with severe OHSS as outpatients by treating them with GnRH antagonists in the luteal phase.
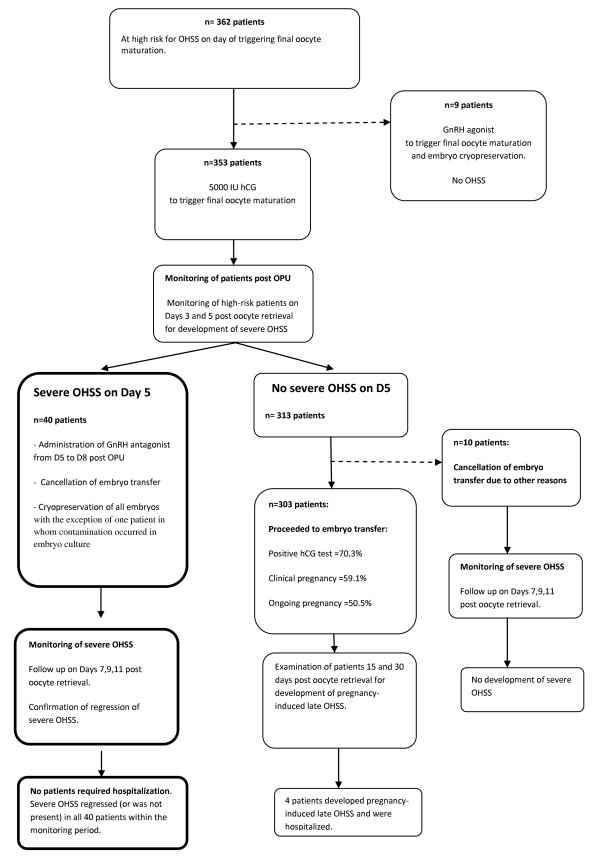
Methods: This is a single-centre, prospective, observational, cohort study. Forty patients diagnosed with severe OHSS, five days post oocyte retrieval, were managed as outpatients after administration of GnRH antagonist (0.25 mg) daily from days 5 to 8 post oocyte retrieval, combined with cryopreservation of all embryos. The primary outcome measure was the proportion of patients with severe OHSS, in whom outpatient management was not feasible.
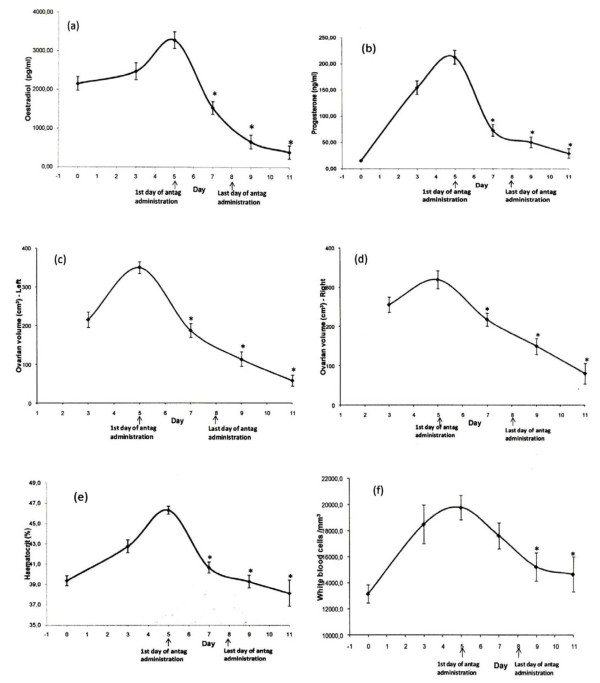
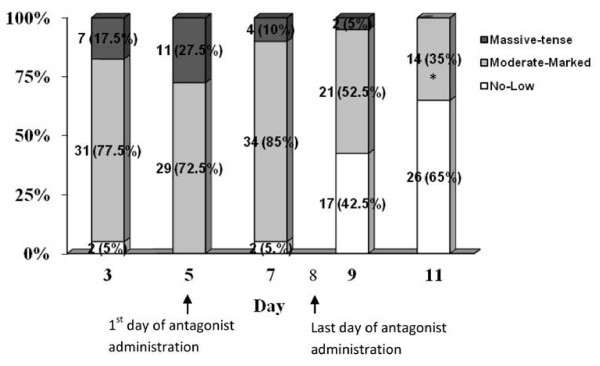
Results: 11.3% (95% CI 8.3%-15.0%) of patients (40/353) developed severe early OHSS. None of the 40 patients required hospitalization following luteal antagonist administration and embryo cryopreservation. Ovarian volume, ascites, hematocrit, WBC, serum oestradiol and progesterone decreased significantly (P < 0.001) by the end of the monitoring period, indicating rapid resolution of severe OHSS.
Conclusions: The current study suggests, for the first time, that successful outpatient management of severe OHSS with antagonist treatment in the luteal phase is feasible and is associated with rapid regression of the syndrome, challenging the dogma of inpatient management. The proposed management is a flexible approach that minimizes unnecessary embryo transfer cancellations in the majority (88.7%) of high risk for OHSS patients.
Figures
References
-
- Lyons CA, Wheeler CA, Frishman GN, Hackett RJ, Seifer DB, Haning RV. Early and late presentation of the ovarian hyperstimulation syndrome: two distinct entities with different risk factors. Hum Reprod. 1994;9(5):792–799. - PubMed
-
- Navot D, Bergh PA, Laufer N. Ovarian hyperstimulation syndrome in novel reproductive technologies: prevention and treatment. Fertil Steril. 1992;58(2):249–261. - PubMed
-
- Aboulghar MA, Mansour RT, Serour GI, Sattar MA, Amin YM, Elattar I. Management of severe ovarian hyperstimulation syndrome by ascitic fluid aspiration and intensive intravenous fluid therapy. Obstet Gynecol. 1993;81(1):108–111. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
