

Treatment of choroid plexus tumors: a 20-year single institutional experience
- PMID: 22938081
- PMCID: PMC4859224
- DOI: 10.3171/2012.8.PEDS12132
Treatment of choroid plexus tumors: a 20-year single institutional experience
Abstract
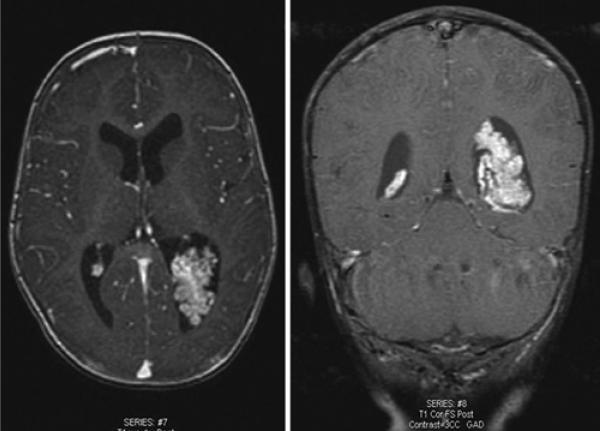
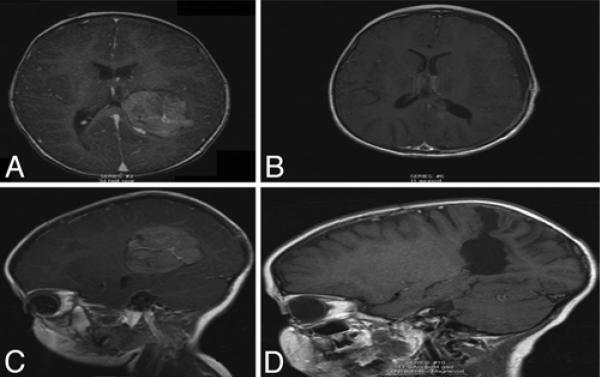
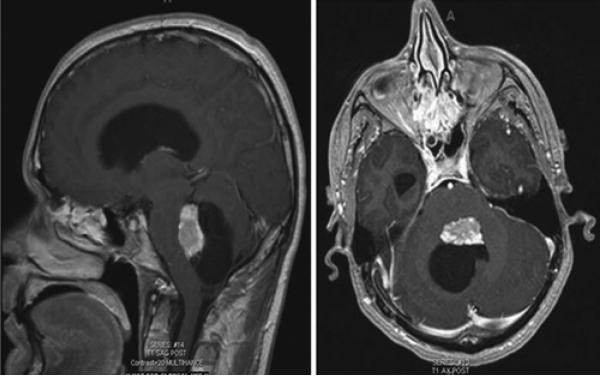
Object: Choroid plexus tumors (CPTs) are rare intracranial neoplasms that constitute approximately 2%-5% of all pediatric brain tumors. Most of these tumors present with severe hydrocephalus. The optimal perioperative management and oncological care remain a matter of debate. The authors present the epidemiological and clinical features of CPTs from a 20-year single-institutional experience.
Methods: A total of 39 consecutive patients with pathologically proven CPTs (31 choroid plexus papillomas [CPPs] and 8 choroid plexus carcinomas [CPCs]) were included in this series. Patient demographics, clinical presentation, comorbidities, indications for surgery, radiological studies, tumor location, and all operative variables were reviewed for each case. Multivariate regression analysis was performed to identify independent predictors of tumor recurrence and survival.
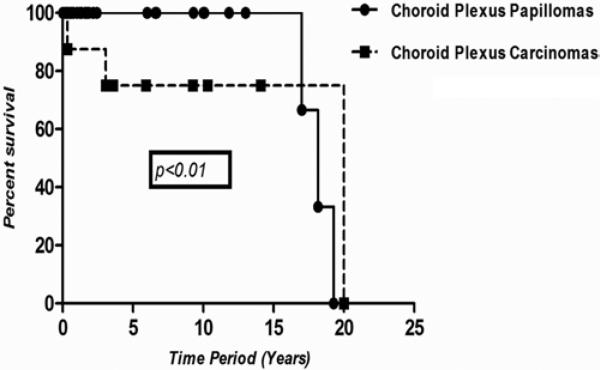
Results: The overall mean age (± SD) was 13.13 ± 19.59 years (15.27 ± 21.10 years in the CPP group and 3.66 ± 3.59 years in the CPC group). Hydrocephalus was noted at presentation in 34% of patients. The most common presenting symptoms were headache (32%) and nausea/vomiting (26%). Gross-total resection (GTR) was achieved in 86% of CPPs and in 71% of CPCs (p = 0.57). There was 100% survival in patients with CPPs observed at the 5- and 10-year follow-up and 71% survival in patients with CPCs at the 5-year follow-up. In a multivariate regression analysis, a diagnosis of papilloma, preoperative vision changes, or hydrocephalus; right ventricle tumor location; and GTR were all independently associated with a decreased likelihood of tumor recurrence at last follow-up.
Conclusions: The authors' study suggests that patients with CPCs are more likely to experience local recurrence and metastasis; hence, GTR with chemotherapy and radiotherapy, particularly for CPCs, is pivotal in preventing recurrence and prolonging survival. While GTR was important for local control following resection of CPPs, it had a minimal effect on prolonging survival in this patient cohort.
Figures
References
-
- Allen J, Wisoff J, Helson L, Pearce J, Arenson E. Choroid plexus carcinoma—responses to chemotherapy alone in newly diagnosed young children. J Neurooncol. 1992;12:69–74. - PubMed
-
- Barbosa M, Rebelo O, Barbosa P, Lacerda A, Fernandes R. Choroid plexus tumours: a surgically treated series. Neurocirugia (Astur) 2001;12:7–16. - PubMed
-
- Berger C, Thiesse P, Lellouch-Tubiana A, Kalifa C, Pierre-Kahn A, Bouffet E. Choroid plexus carcinomas in childhood: clinical features and prognostic factors. Neurosurgery. 1998;42:470–475. - PubMed
-
- Boyd MC, Steinbok P. Choroid plexus tumors: problems in diagnosis and management. J Neurosurg. 1987;66:800–805. - PubMed
-
- Chow E, Reardon DA, Shah AB, Jenkins JJ, Langston J, Heideman RL, et al. Pediatric choroid plexus neoplasms. Int J Radiat Oncol Biol Phys. 1999;44:249–254. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
