

Examining and mitigating acellular hemoglobin vasoactivity
- PMID: 22938394
- PMCID: PMC3638537
- DOI: 10.1089/ars.2012.4922
Examining and mitigating acellular hemoglobin vasoactivity
Abstract
Significance: There has been a striking advancement in our understanding of red cell substitutes over the past decade. Although regulatory oversight has influenced many aspects of product development in this period, those who have approached the demonstration of efficacy of red cell substitutes have failed to understand their implication at the level of the microcirculation, where blood interacts closely with tissue.
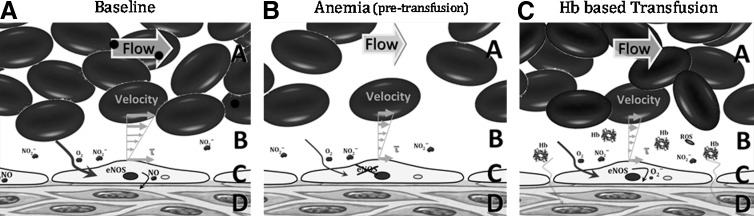
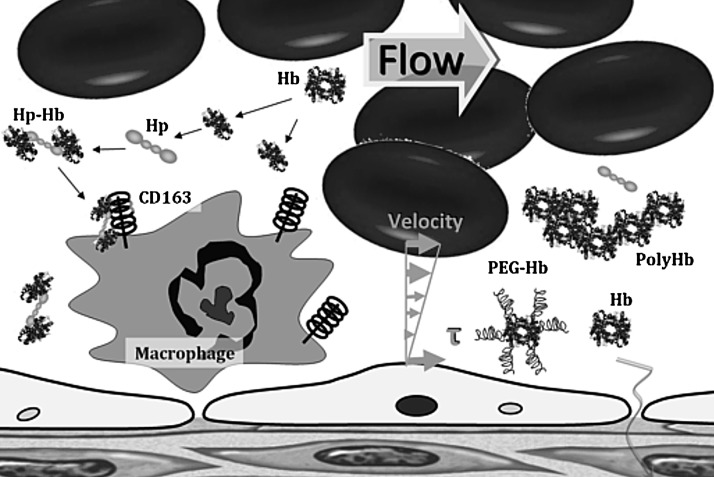
Recent advances: The understanding of the adverse effects of acellular hemoglobin (Hb)-based oxygen carriers (HBOCs) has fortunately expanded from Hb-induced renal toxicity to a more complete list of biochemical mechanism. In addition, various unexpected adverse reactions were seen in early clinical studies. The effects of the presence of acellular Hb in plasma are relatively unique because of the convergence of mechanical and biochemical natures.
Critical issues: Controlling the variables using genetic engineering and chemical modification to change specific characteristics of the Hb molecule may allow for solving the complex multivariate problems of acellular Hb vasoactivity. HBOCs may never be rendered free of negative effects; however, quantifying the nature and extent of microvascular complications establishes a platform for designing new ameliorative therapies.
Future directions: It is time to leave behind the study of vasoactivity and toxicity based on bench-top measurements of biochemical changes and those based solely on systemic parameters in vivo, and move to a more holistic analysis of the mechanisms creating the problems, complemented with meaningful studies of efficacy.
Figures



References
-
- Medical expenditures attributable to injuries—United States, 2000. MMWR Morb Mortal Wkly Rep. 2004;53:1–4. - PubMed
-
- Global Database on Blood Safety. Geneva: World Health Organization; 2008. Report 2004–2005.
-
- Alayash AI. Hemoglobin-based blood substitutes: oxygen carriers, pressor agents, or oxidants? Nat Biotechnol. 1999;17:545–549. - PubMed
-
- Alayash AI. Hemoglobin-based blood substitutes and the hazards of blood radicals. Free Radic Res. 2000;33:341–348. - PubMed
-
- Alayash AI. Oxygen therapeutics: can we tame haemoglobin? Nat Rev Drug Disc. 2004;3:152–159. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
