

The effect of depression on stage at diagnosis, treatment, and survival in pancreatic adenocarcinoma
- PMID: 22938900
- PMCID: PMC3465163
- DOI: 10.1016/j.surg.2012.06.010
The effect of depression on stage at diagnosis, treatment, and survival in pancreatic adenocarcinoma
Abstract
Background: Depression has been associated with delayed presentation, inadequate treatment, and poor survival in patients with cancer.
Methods: Using Surveillance, Epidemiology and End Results and Medicare linked data (1992-2005), we identified patients with pancreatic adenocarcinoma (N = 23,745). International classification of diseases, 9th edition, clinical modification codes were used to evaluate depression during the 3 to 27 months before the diagnosis of cancer. The effect of depression on receipt of therapy and survival was evaluated in univariate and multivariate models.
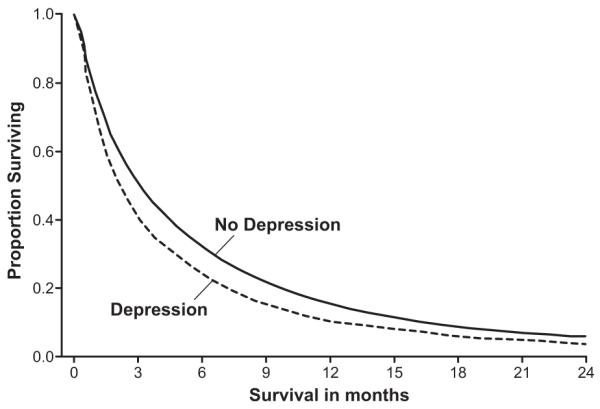
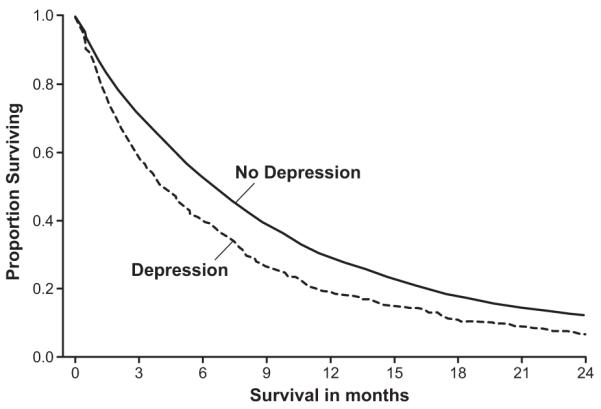
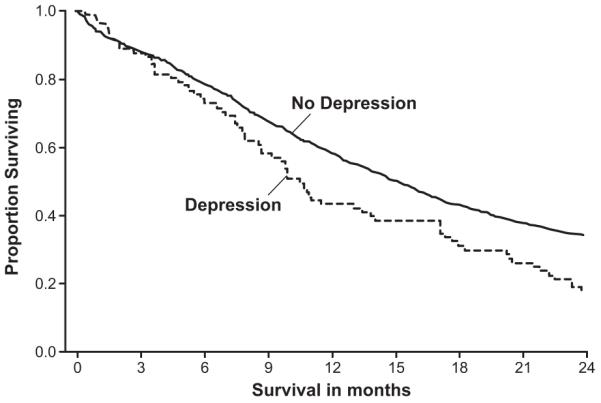
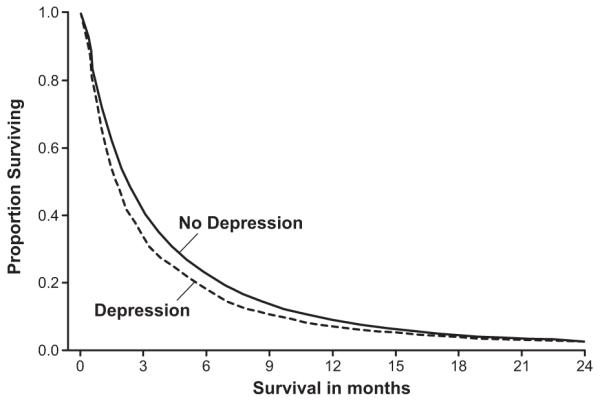
Results: Of patients with pancreatic cancer in our study, 7.9% had a diagnosis of depression (N = 1,868). Depression was associated with increased age, female sex, white race, single or widowed status, and advanced stage disease (P < .0001). In an adjusted model, patients with locoregional disease and depression had 37% lower odds of undergoing surgical resection (odds ratio, 0.63; 95% confidence interval, 0.52-0.76). In patients with locoregional disease, depression was associated with lower 2-year survival (hazard ratio, 1.20; 95% confidence interval, 1.09-1.32). After adjusting for surgical resection, this association was attenuated (hazard ratio, 1.14; 95% confidence interval, 1.04-1.26). In patients who underwent surgical resection, depression was a significant predictor of survival (hazard ratio, 1.34; 95% confidence interval, 1.04-1.73). Patients with distant disease and depression had 21% lower odds of receiving chemotherapy (odds ratio, 0.79; 95% confidence interval, 0.70-0.90). After adjusting for chemotherapy for distant disease, depression was no longer a significant predictor of survival (hazard ratio, 1.03; 95% confidence interval, 0.97-1.09).
Conclusion: The decreased survival associated with depression appears to be mediated by a lower likelihood of appropriate treatment in depressed patients. Accurate recognition and treatment of pancreatic cancer patients with depression may improve treatment rates and survival.
Copyright © 2012 Mosby, Inc. All rights reserved.
Figures
Similar articles
-
Racial differences in cancer specialist consultation, treatment, and outcomes for locoregional pancreatic adenocarcinoma.Ann Surg Oncol. 2009 Nov;16(11):2968-77. doi: 10.1245/s10434-009-0656-5. Epub 2009 Aug 11. Ann Surg Oncol. 2009. PMID: 19669839
-
Effects of depression on the survival of pancreatic adenocarcinoma.Pancreas. 2006 Jan;32(1):58-61. doi: 10.1097/01.mpa.0000191643.17173.d3. Pancreas. 2006. PMID: 16340745
-
Associations of Socioeconomic Variables With Resection, Stage, and Survival in Patients With Early-Stage Pancreatic Cancer.JAMA Surg. 2016 Apr;151(4):338-45. doi: 10.1001/jamasurg.2015.4239. JAMA Surg. 2016. PMID: 26581025
-
Prognostic factors in ductal pancreatic cancer.Langenbecks Arch Surg. 1998 Apr;383(2):129-33. doi: 10.1007/s004230050104. Langenbecks Arch Surg. 1998. PMID: 9641885 Review.
-
Pancreatic Adenocarcinoma: Trends in Epidemiology, Risk Factors, and Outcomes.Hematol Oncol Clin North Am. 2022 Oct;36(5):879-895. doi: 10.1016/j.hoc.2022.07.002. Epub 2022 Sep 23. Hematol Oncol Clin North Am. 2022. PMID: 36154788 Free PMC article. Review.
Cited by
-
Depression and Health Care Utilization at End of Life Among Older Adults With Advanced Non-Small-Cell Lung Cancer.J Pain Symptom Manage. 2018 Nov;56(5):699-708.e1. doi: 10.1016/j.jpainsymman.2018.08.004. Epub 2018 Aug 17. J Pain Symptom Manage. 2018. PMID: 30121375 Free PMC article.
-
Association Between Depression and Anxiety Status With Uptake of Colorectal Cancer Screening Among US Adults: A Population-Level Study.Cureus. 2023 Jul 29;15(7):e42659. doi: 10.7759/cureus.42659. eCollection 2023 Jul. Cureus. 2023. PMID: 37644921 Free PMC article.
-
The effect of a severe psychiatric illness on colorectal cancer treatment and survival: A population-based retrospective cohort study.PLoS One. 2020 Jul 29;15(7):e0235409. doi: 10.1371/journal.pone.0235409. eCollection 2020. PLoS One. 2020. PMID: 32726314 Free PMC article.
-
Diagnostic Performance of the 4-Item Geriatric Depression Scale for Depression Screening in Older Patients with Cancer: The ELCAPA Cohort Study.Oncologist. 2021 Jun;26(6):e983-e991. doi: 10.1002/onco.13746. Epub 2021 Mar 23. Oncologist. 2021. PMID: 33683759 Free PMC article.
-
Cancer Mortality in People Treated with Antidepressants before Cancer Diagnosis: A Population Based Cohort Study.PLoS One. 2015 Sep 14;10(9):e0138134. doi: 10.1371/journal.pone.0138134. eCollection 2015. PLoS One. 2015. PMID: 26367120 Free PMC article.
References
-
- Himelhoch S, Weller WE, Wu AW, et al. Chronic medical illness, depression, and use of acute medical services among Medicare beneficiaries. Med Care. 2004;42:512–21. - PubMed
-
- McCall NT, Parks P, Smith K, et al. The prevalence of major depression or dysthymia among aged Medicare Fee-for-Service beneficiaries. Int J Geriatr Psychiatry. 2002;17:557–65. - PubMed
-
- Stordal E, Bjartveit Kruger M, Dahl NH, et al. Depression in relation to age and gender in the general population: the Nord-Trondelag Health Study (HUNT) Acta Psychiatr Scand. 2001;104:210–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
