

Characteristics of patients with cardiorespiratory instability in a step-down unit
- PMID: 22941708
- PMCID: PMC3679534
- DOI: 10.4037/ajcc2012797
Characteristics of patients with cardiorespiratory instability in a step-down unit
Abstract
Background: Patients in step-down units are at higher risk for developing cardiorespiratory instability than are patients in general care areas. A triage tool is needed to identify at-risk patients who therefore require increased surveillance.
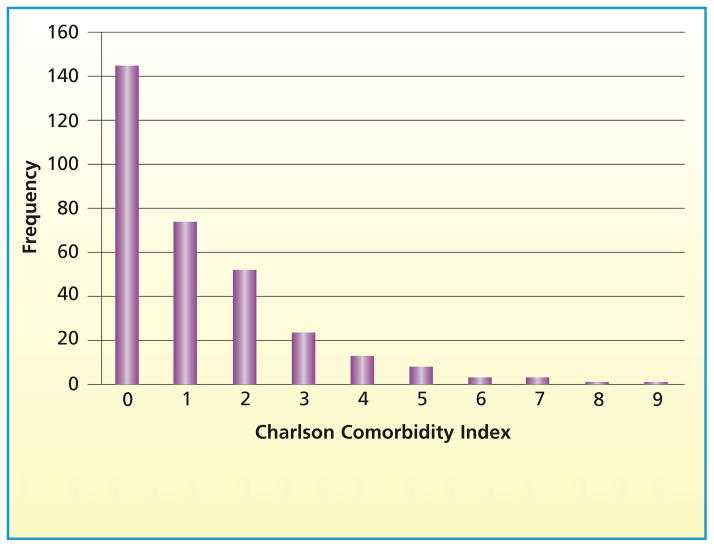
Objectives: To determine demographic (age, race, sex) and clinical (Charlson Comorbidity Index at admission, admitting diagnosis, care area of origin, admission service) differences between patients in step-down units who did and did not experience cardiorespiratory instability.
Methods: In a prospective longitudinal pilot study, 326 surgical-trauma patients had continuous monitoring of heart rate, respirations, and oxygen saturation and intermittent noninvasive measurement of blood pressure. Cardiorespiratory instability was defined as heart rate less than 40/min or greater than 140/min, respirations less than 8/min or greater than 36/min, oxygen saturation less than 85%, or blood pressure less than 80 or greater than 200 mm Hg systolic or greater than 110 mm Hg diastolic. Patients' status was classified as unstable if their values crossed these thresholds even once during their stay.
Results: Cardiorespiratory instability occurred in 34% of patients. The Charlson Comorbidity Index was the only variable associated with instability conditions. Compared with patients with no comorbid conditions (50%), more patients with at least 1 comorbid condition (66%) experienced instability (P = .006). Each 1-unit increase in the Charlson Index increased the odds for cardiorespiratory instability by 1.17 (P = .03).
Conclusion: Although the relationship between Charlson Comorbidity Index and cardiorespiratory instability was weak, adding it to current surveillance systems might improve detection of instability.
Figures
References
-
- Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288:1987–1993. - PubMed
-
- DeVita MA, Bellomo R, Hillman K, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med. 2006;34(9):2463–2478. - PubMed
