

An integrated approach in the diagnosis of smoking-related interstitial lung diseases
- PMID: 22941885
- PMCID: PMC9487338
- DOI: 10.1183/09059180.00003112
An integrated approach in the diagnosis of smoking-related interstitial lung diseases
Abstract
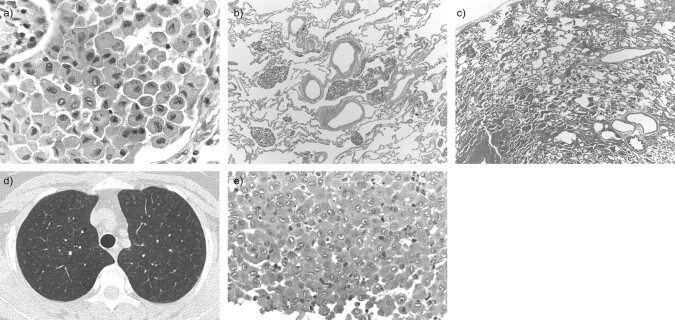
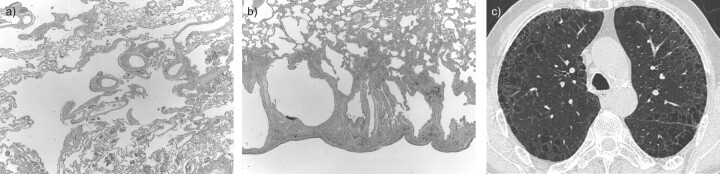
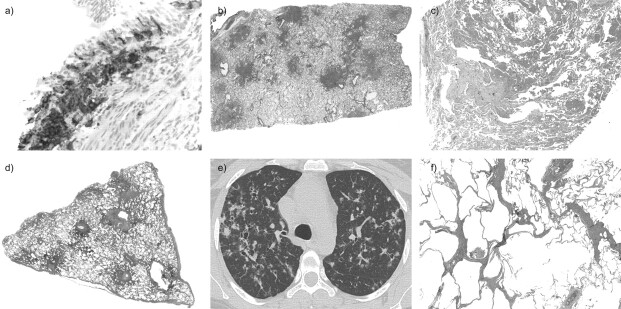
Cigarette smoke consists of several chemical compounds with a variety of effects in many organs. In the lung, apart being the main cause of chronic obstructive pulmonary disease, carcinoma and idiopathic spontaneous pneumothorax, tobacco smoke is associated with interstitial lung diseases (ILDs), including respiratory bronchiolitis-associated ILD (RB-ILD), desquamative interstitial pneumonia (DIP), pulmonary Langerhans' cell histiocytosis (PLCH), idiopathic pulmonary fibrosis, acute eosinophilic pneumonia, ILD in rheumatoid arthritis and pulmonary haemorrhage in Goodpasture syndrome. This review will focus on the diseases with a stronger epidemiological association with tobacco smoke, namely RB-ILD, DIP and PLCH. Although the exact pathogenetic evidence linking smoking with these disorders is still not completely understood, there is growing evidence that tobacco smoke targets the terminal or respiratory bronchioles in these diseases, and the differences are reflective of the degree of severity of small airway and parenchymal reaction to the smoke exposure. Despite considerable clinical, radiological and histological overlap between RB-ILD, DIP and PLCH, it is useful to retain the separate classifications for prognostic and therapeutic implications.
Conflict of interest statement
S. Harari has relationships with drug companies including Actelion, InterMune and GSK. In addition to being an investigator in trials involving these companies, relationships include consultancy service and membership of scientific advisory boards.
Figures
Comment in
-
Global effort against rare and orphan diseases.Eur Respir Rev. 2012 Sep 1;21(125):171-2. doi: 10.1183/09059180.00004112. Eur Respir Rev. 2012. PMID: 22941880 Free PMC article. No abstract available.
References
-
- Visscher DW, Myers JL. Bronchiolitis: the pathologist's perspective. Proc Am Thorac Soc 2006; 3: 41–47. - PubMed
-
- Wright JL, Cagle P, Churg A, et al. Diseases of the small airways. Am Rev Respir Dis 1992; 146: 240–262. - PubMed
-
- Shaw RJ, Djukanovic R, Tashkin DP, et al. The role of small airways in lung disease. Respir Med 2002; 96: 67–80. - PubMed
-
- Fraig M, Shreesha U, Savici D, et al. Respiratory bronchiolitis: a clinicopathologic study in current smokers, ex-smokers, and never-smokers. Am J Surg Pathol 2002; 26: 647–653. - PubMed
-
- Myers JL, Veal CF, Jr, Shin MS, et al. Respiratory bronchiolitis causing interstitial lung disease: a clinical pathologic study of six cases. Am Rev Respir Dis 1987; 135: 880–884. - PubMed