

Long-term follow-up of the multicenter, multidisciplinary treatment study HIT-LGG-1996 for low-grade glioma in children and adolescents of the German Speaking Society of Pediatric Oncology and Hematology
- PMID: 22942186
- PMCID: PMC3452343
- DOI: 10.1093/neuonc/nos202
Long-term follow-up of the multicenter, multidisciplinary treatment study HIT-LGG-1996 for low-grade glioma in children and adolescents of the German Speaking Society of Pediatric Oncology and Hematology
Abstract
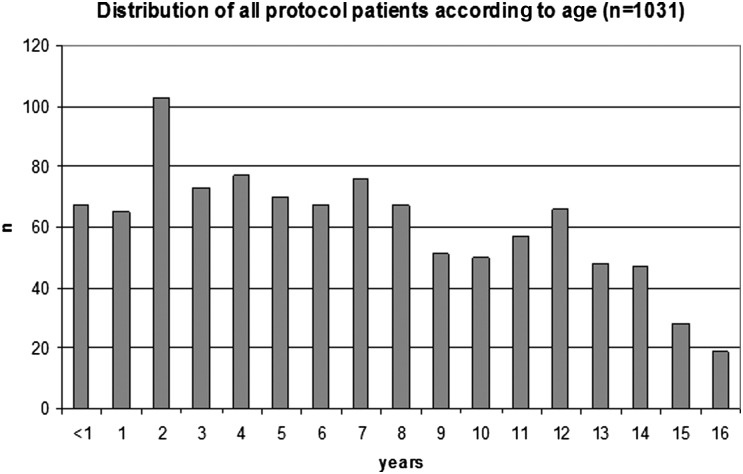
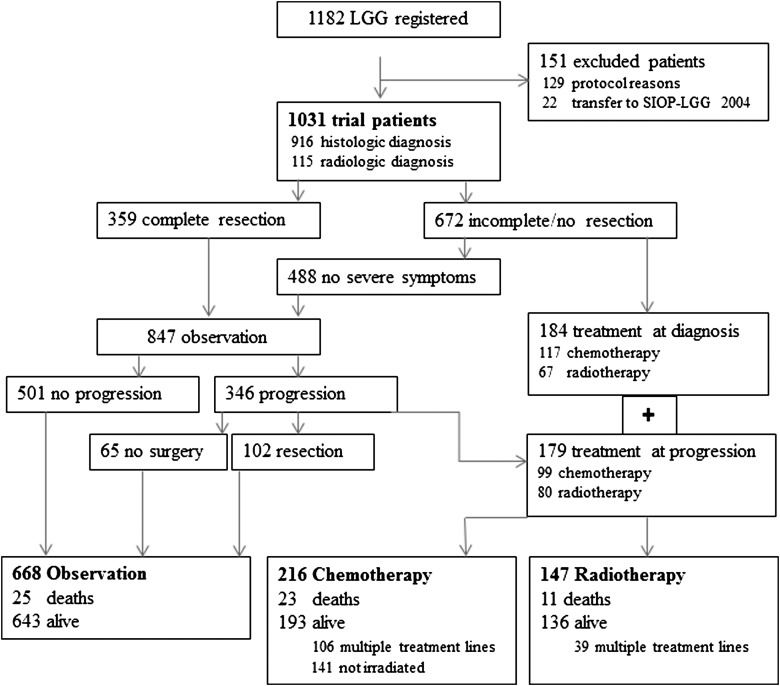
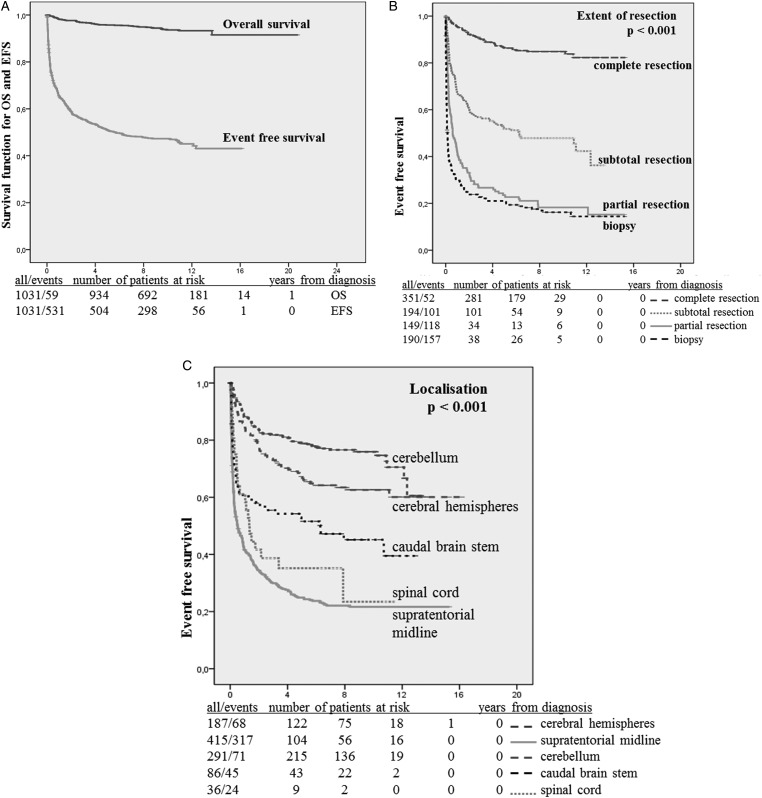
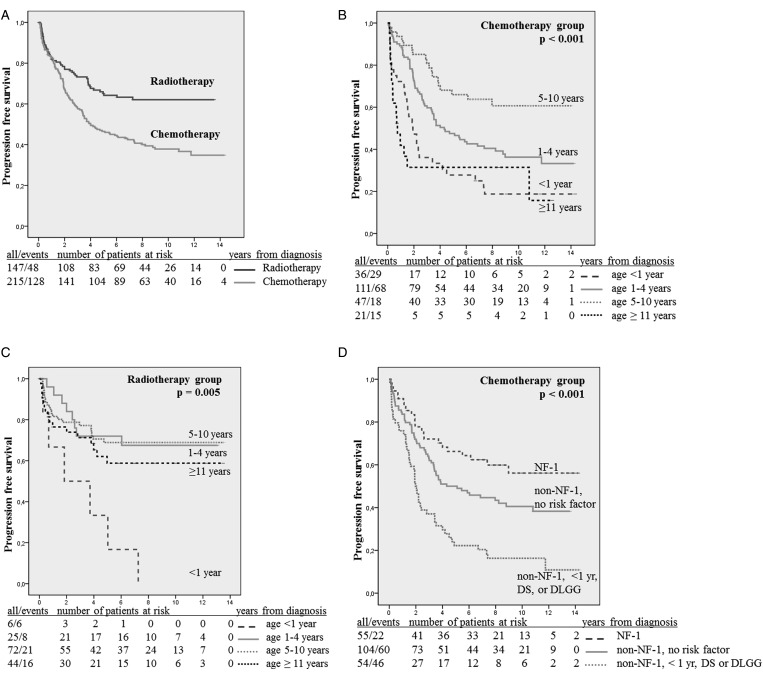
The Hirntumorstudien (HIT)-LGG-1996 protocol offered a comprehensive treatment strategy for pediatric patients with low-grade glioma (LGG), ie, observation, surgery, adjuvant radiotherapy, and chemotherapy to defer the start of irradiation in young children. In this current study, we sought to determine clinical factors for progression and survival. Between October 1, 1996 and March 31, 2004, 1031 patients were prospectively recruited into an observation arm (n = 668) and a nonsurgical arm stratifying 12 months of vincristine-carboplatin chemotherapy (n = 216) and conventional radiotherapy/brachytherapy (n = 147) in an age-dependent manner. Median patient age was 6.9 years; 28 patients had diencephalic syndrome, 44 had dissemination, and 108 had neurofibromatosis type 1(NF-1). Main tumor location was the supratentorial midline (40.4%), and the main histology was pilocytic astrocytoma (67.9%). Following a median observation of 9.3 years, 10-year overall survival (OS) was 0.94 and 10-year event-free survival (EFS) was 0.47. Ten-year progression-free survival was 0.62 following radiotherapy and 0.44 following chemotherapy. Sixty-one of 216 chemotherapy patients received radiotherapy 0.3-8.7 years after initial diagnosis. By multivariate analysis, diencephalic syndrome and incomplete resection were found to be unfavorable factors for OS and EFS, age ≥11 years for OS, and supratentorial midline location for EFS. Dissemination, age <1 year, and nonpilocytic histology were unfavorable factors for progression following radiotherapy (138 patients); and diencephalic syndrome, dissemination, and age ≥11 years were unfavorable factors following chemotherapy (210 patients). NF-1 patients and boys experienced prolonged tumor stabilization with chemotherapy. A nationwide multimodal treatment strategy is feasible for pediatric LGG. Extended follow-up yielded results comparable to single-institution series for the treatment groups. Three-quarters of surviving chemotherapy patients have not yet received radiation therapy. Infants with or without diencephalic syndrome and dissemination bear the highest risk for death and progression following diagnosis or treatment.
Figures
References
-
- Abdollahzadeh M, Hoffman HJ, Blazer SI, et al. Benign cerebellar astrocytoma in childhood: experience at the Hospital for Sick Children 1980–1992. Childs Nerv Syst. 1994;10(6):380–383. - PubMed
-
- Berger MS, Deliganis AV, Dobbins J, Keles GE. The effect of extent of resection on recurrence in patients with low grade cerebral hemisphere gliomas. Cancer. 1994;74(6):1784–1791. - PubMed
-
- Campbell JW, Pollack IF. Cerebellar astrocytomas in children. J Neurooncol. 1996;28(2–3):223–231. - PubMed
-
- Constantini S, Houten J, Miller DC, et al. Intramedullary spinal cord tumors in children under the age of 3 years. J Neurosurg. 1996;85(6):1036–1043. - PubMed
-
- Pollack IF, Claassen D, al-Shboul Q, Janosky JE, Deutsch M. Low-grade gliomas of the cerebral hemispheres in children: an analysis of 71 cases. J Neurosurg. 1995;82(4):536–547. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
