

Predictors of hypocretin (orexin) deficiency in narcolepsy without cataplexy
- PMID: 22942503
- PMCID: PMC3413802
- DOI: 10.5665/sleep.2080
Predictors of hypocretin (orexin) deficiency in narcolepsy without cataplexy
Abstract
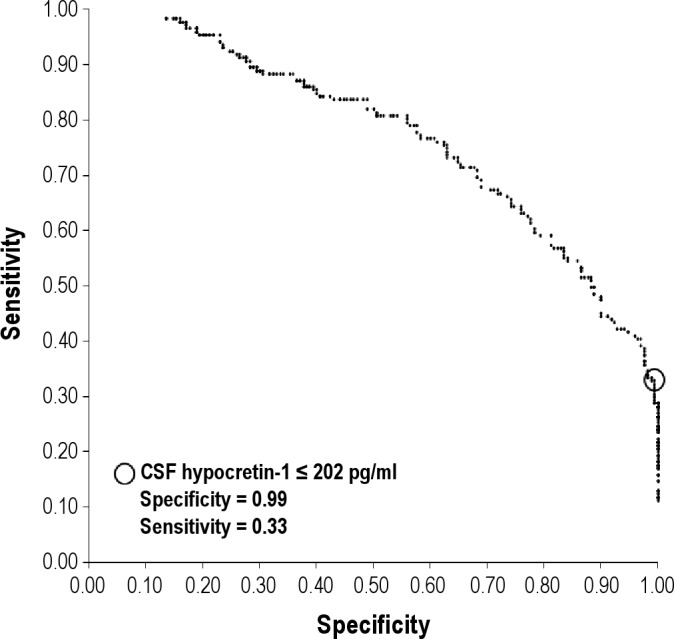
Study objectives: To compare clinical, electrophysiologic, and biologic data in narcolepsy without cataplexy with low (≤ 110 pg/ml), intermediate (110-200 pg/ml), and normal (> 200 pg/ml) concentrations of cerebrospinal fluid (CSF) hypocretin-1.
Setting: University-based sleep clinics and laboratories.
Patients: Narcolepsy without cataplexy (n = 171) and control patients (n = 170), all with available CSF hypocretin-1.
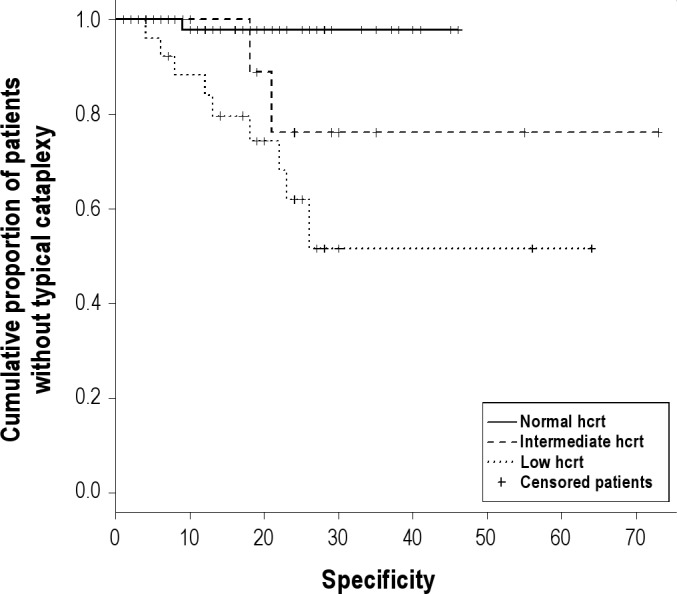
Design and interventions: Retrospective comparison and receiver operating characteristics curve analysis. Patients were also recontacted to evaluate if they developed cataplexy by survival curve analysis.
Measurements and results: The optimal cutoff of CSF hypocretin-1 for narcolepsy without cataplexy diagnosis was 200 pg/ml rather than 110 pg/ml (sensitivity 33%, specificity 99%). Forty-one patients (24%), all HLA DQB1*06:02 positive, had low concentrations (≤ 110 pg/ml) of CSF hypocretin-1. Patients with low concentrations of hypocretin-1 only differed subjectively from other groups by a higher Epworth Sleepiness Scale score and more frequent sleep paralysis. Compared with patients with normal hypocretin-1 concentration (n = 117, 68%), those with low hypocretin-1 concentration had higher HLA DQB1*06:02 frequencies, were more frequently non-Caucasians (notably African Americans), with lower age of onset, and longer duration of illness. They also had more frequently short rapid-eye movement (REM) sleep latency (≤ 15 min) during polysomnography (64% versus 23%), and shorter sleep latencies (2.7 ± 0.3 versus 4.4 ± 0.2 min) and more sleep-onset REM periods (3.6 ± 0.1 versus 2.9 ± 0.1 min) during the Multiple Sleep Latency Test (MSLT). Patients with intermediate concentrations of CSF hypocretin-1 (n = 13, 8%) had intermediate HLA DQB1*06:02 and polysomnography results, suggesting heterogeneity. Of the 127 patients we were able to recontact, survival analysis showed that almost half (48%) with low concentration of CSF hypocretin-1 had developed typical cataplexy at 26 yr after onset, whereas only 2% had done so when CSF hypocretin-1 concentration was normal. Almost all patients (87%) still complained of daytime sleepiness independent of hypocretin status.
Conclusion: Objective (HLA typing, MSLT, and sleep studies) more than subjective (sleepiness and sleep paralysis) features predicted low concentration of CSF hypocretin-1 in patients with narcolepsy without cataplexy.
Keywords: Hypocretin; MSLT; REM latency; low CSF-hypocretin-1; narcolepsy without cataplexy; polysomnography.
Figures
Similar articles
-
Nocturnal rapid eye movement sleep latency for identifying patients with narcolepsy/hypocretin deficiency.JAMA Neurol. 2013 Jul;70(7):891-902. doi: 10.1001/jamaneurol.2013.1589. JAMA Neurol. 2013. PMID: 23649748 Free PMC article.
-
The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias.Arch Neurol. 2002 Oct;59(10):1553-62. doi: 10.1001/archneur.59.10.1553. Arch Neurol. 2002. PMID: 12374492
-
Narcolepsy without cataplexy: 2 subtypes based on CSF hypocretin-1/orexin-A findings.Sleep. 2006 Nov;29(11):1439-43. doi: 10.1093/sleep/29.11.1439. Sleep. 2006. PMID: 17162990
-
Symptomatic narcolepsy, cataplexy and hypersomnia, and their implications in the hypothalamic hypocretin/orexin system.Sleep Med Rev. 2005 Aug;9(4):269-310. doi: 10.1016/j.smrv.2005.03.004. Sleep Med Rev. 2005. PMID: 16006155 Review.
-
[Moebius syndrome and narcolepsy].Nervenarzt. 2014 Dec;85(12):1569-72. doi: 10.1007/s00115-014-4174-8. Nervenarzt. 2014. PMID: 25388761 Review. German.
Cited by
-
Narcolepsy: clinical differences and association with other sleep disorders in different age groups.J Neurol. 2013 Mar;260(3):767-75. doi: 10.1007/s00415-012-6702-4. Epub 2012 Oct 16. J Neurol. 2013. PMID: 23070467
-
The autoimmune basis of narcolepsy.Curr Opin Neurobiol. 2013 Oct;23(5):767-73. doi: 10.1016/j.conb.2013.04.013. Epub 2013 May 29. Curr Opin Neurobiol. 2013. PMID: 23725858 Free PMC article. Review.
-
Management Of Excessive Sleepiness In Patients With Narcolepsy And OSA: Current Challenges And Future Prospects.Nat Sci Sleep. 2019 Oct 23;11:241-252. doi: 10.2147/NSS.S218402. eCollection 2019. Nat Sci Sleep. 2019. PMID: 31695533 Free PMC article.
-
Narcolepsy: neural mechanisms of sleepiness and cataplexy.J Neurosci. 2012 Sep 5;32(36):12305-11. doi: 10.1523/JNEUROSCI.2630-12.2012. J Neurosci. 2012. PMID: 22956821 Free PMC article. Review. No abstract available.
-
An association analysis of HLA-DQB1 with narcolepsy without cataplexy and idiopathic hypersomnia with/without long sleep time in a Japanese population.Hum Genome Var. 2015 Sep 17;2:15031. doi: 10.1038/hgv.2015.31. eCollection 2015. Hum Genome Var. 2015. PMID: 27081540 Free PMC article.
References
-
- Oka Y, Inoue Y, Kanbayashi T, et al. Narcolepsy without cataplexy: 2 subtypes based on CSF hypocretin-1/orexin-A findings. Sleep. 2006;29:1439–43. - PubMed
-
- Hong SC, Lin L, Jeong JH, et al. A study of the diagnostic utility of HLA typing, CSF hypocretin-1 measurements, and MSLT testing for the diagnosis of narcolepsy in 163 Korean patients with unexplained excessive daytime sleepiness. Sleep. 2006;29:1429–38. - PubMed
-
- Mignot E, Hayduk R, Black J, Grumet FC, Guilleminault C. HLA DQB1*0602 is associated with cataplexy in 509 narcoleptic patients. Sleep. 1997;20:1012–20. - PubMed
-
- Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355:39–40. - PubMed
-
- Mignot E, Lammers GJ, Ripley B, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol. 2002;59:1553–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
