

doi: 10.3978/j.issn.2078-6891.2012.030.
Colorectal carcinoma: Pathologic aspects
Affiliations
- PMID: 22943008
- PMCID: PMC3418538
- DOI: 10.3978/j.issn.2078-6891.2012.030
Item in Clipboard
Colorectal carcinoma: Pathologic aspects
J Gastrointest Oncol.
2012 Sep.
Abstract
Colorectal carcinoma is one of the most common cancers and one of the leading causes of cancer-related death in the United States. Pathologic examination of biopsy, polypectomy and resection specimens is crucial to appropriate patient managemnt, prognosis assessment and family counseling. Molecular testing plays an increasingly important role in the era of personalized medicine. This review article focuses on the histopathology and molecular pathology of colorectal carcinoma and its precursor lesions, with an emphasis on their clinical relevance.
Keywords: BRAF; Colorectal carcinoma; KRAS; MSI; adenoma; molecular; pathology.
Figures
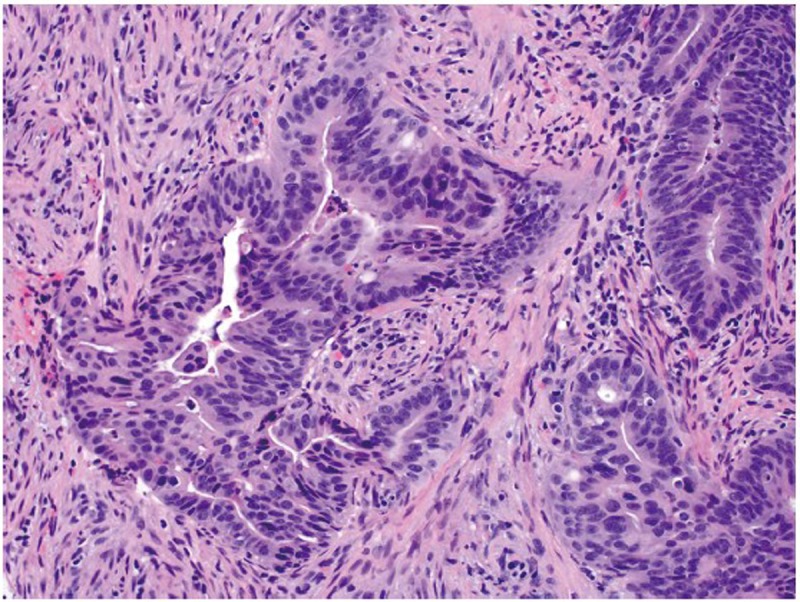
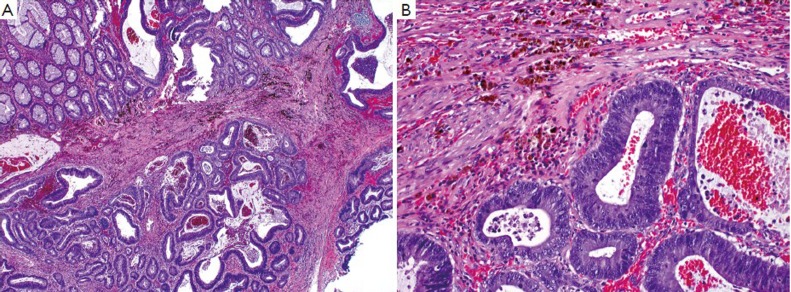
An example of moderately differentiated adenocarcinoma showing complicated glandular structures in a desmoplastic stroma (original magnification ×200)
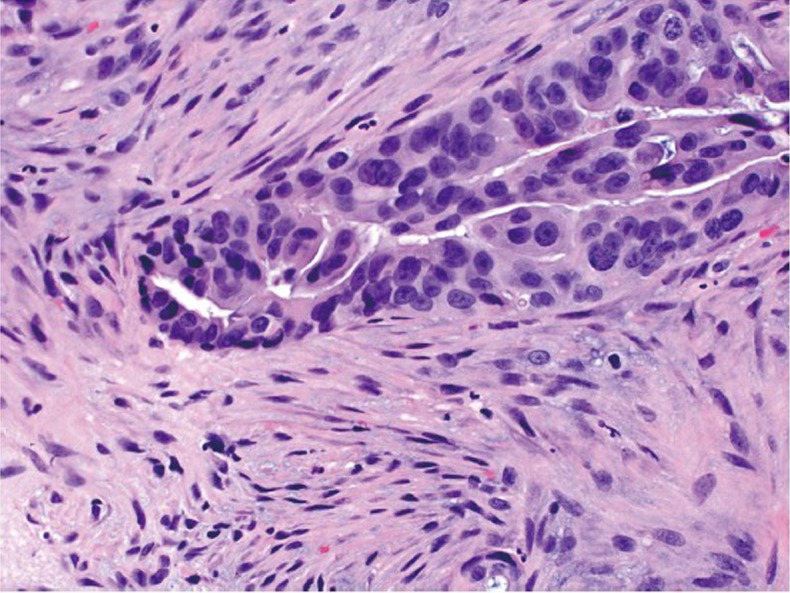
Desmoplastic reaction characterized by proliferation of spindle cells surrounding an adenocarcinomatous gland (original magnification ×400)
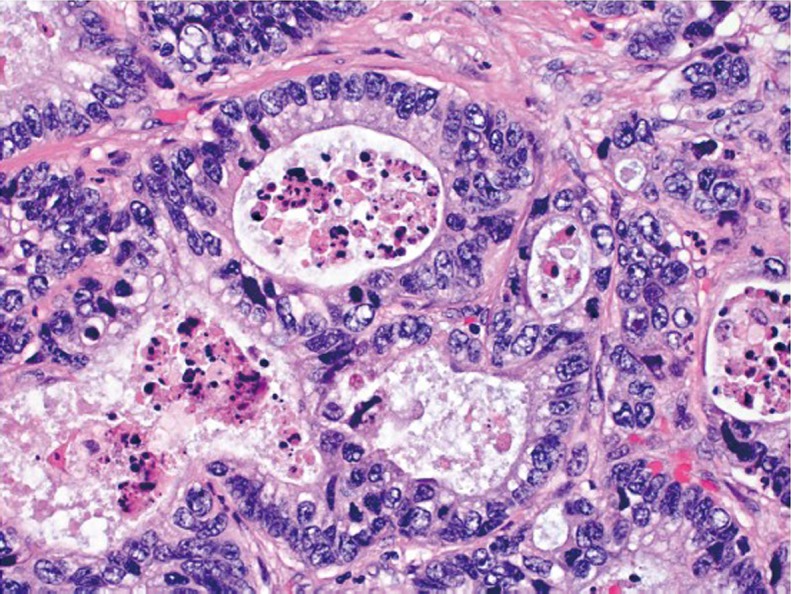
Necrotic debris (“dirty necrosis”) within the lumina of adenocarcinomatous glands (original magnification ×400)
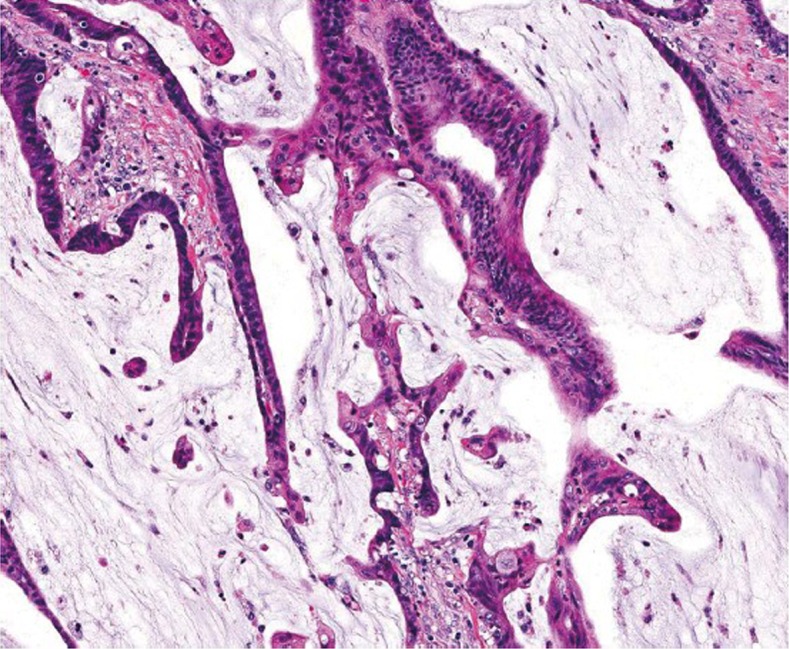
Mucinous adenocarcinoma showing abundant extracellular mucin (original magnification ×200)
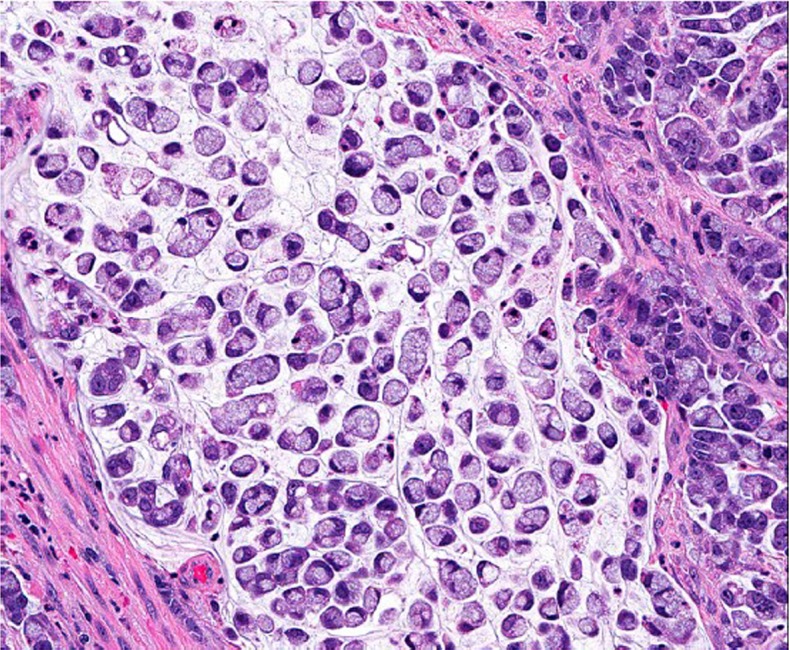
Signet ring cell carcinoma (original magnification ×400)
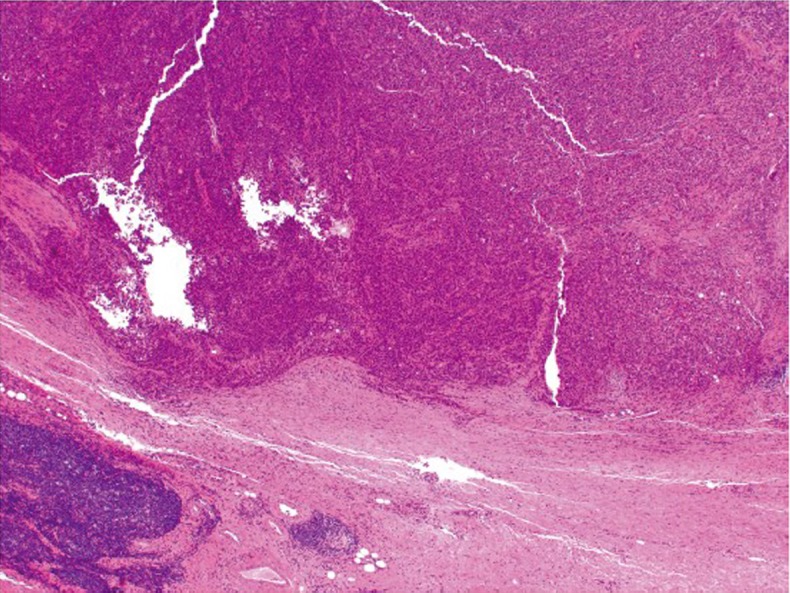
Medullary carcinoma showing a pushing border at the tumor edge (original magnification ×40)
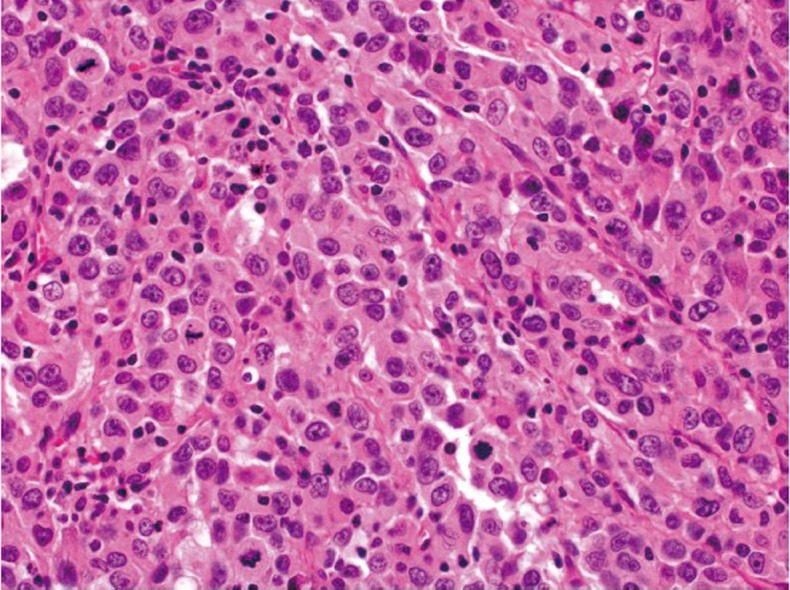
Medullary carcinoma showing poorly differentiated histology and tumor-infiltrating lymphocytes (original magnification ×400)
Tumor cells close to, but not at, the serosal surface, with mesothelial inflammatory and hyperplastic reactions, which may be considered T4a by some investigators (original magnification ×40)
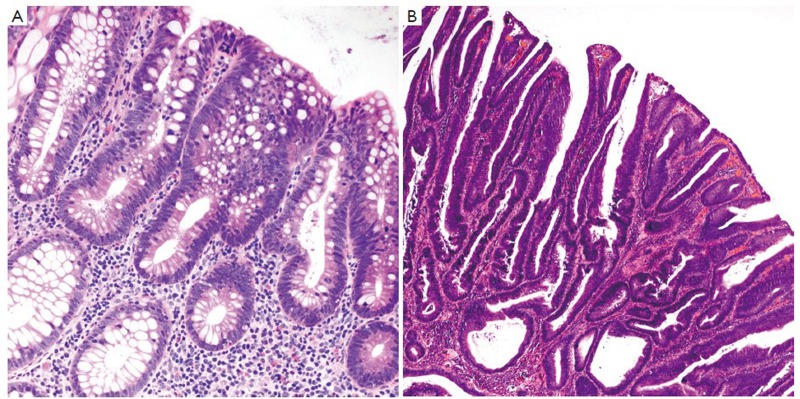
Examples of tubular adenoma (A. original magnification ×200), and tubulovillous adenoma (B. original magnification ×100)
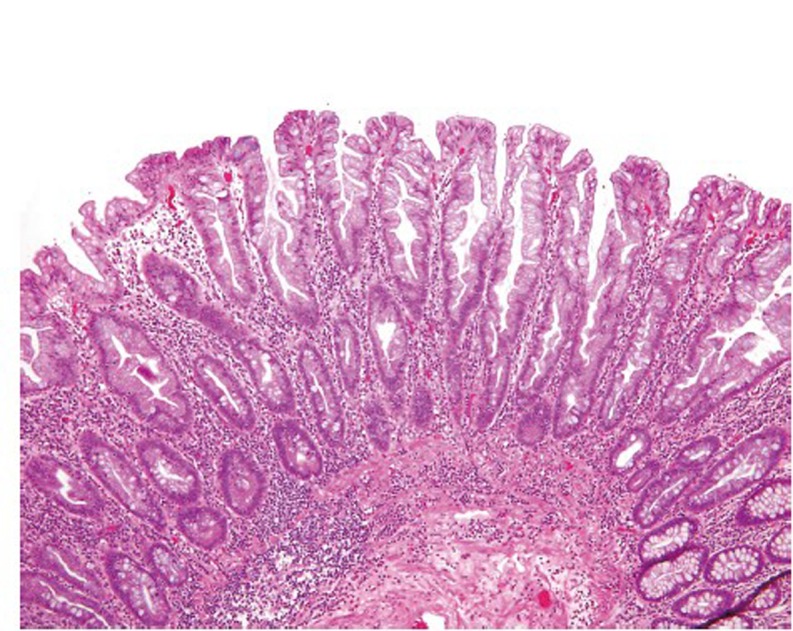
Hyperplastic polyp (original magnification ×100)
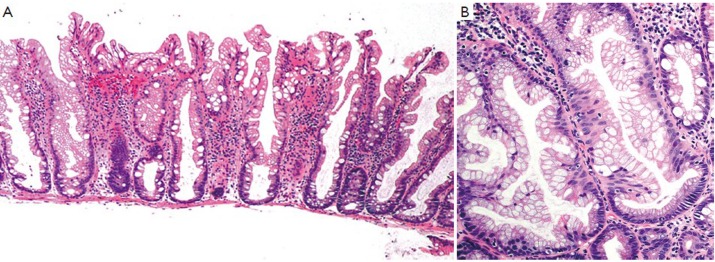
Low power (A. original magnification ×40) and high power (B. original magnification ×200) views of sessile serrated polyp. Note the presence of basal serration
An example of traditional serrated adenoma (original magnification ×400). Note the presence of luminal serration, low grade cytologic dysplasia and cytologic eosinophilia
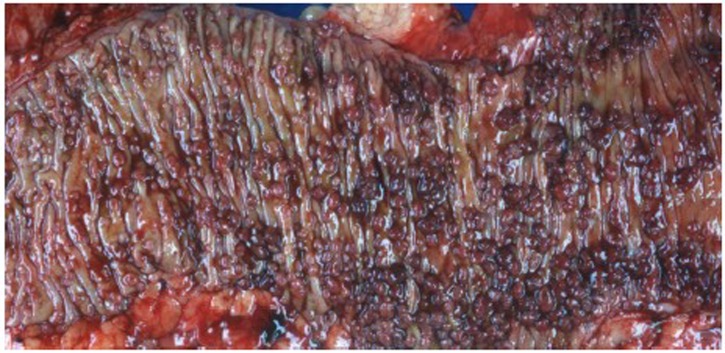
A case of familial adenomatous polyposis. Note the presence of innumerable polyps in the colon
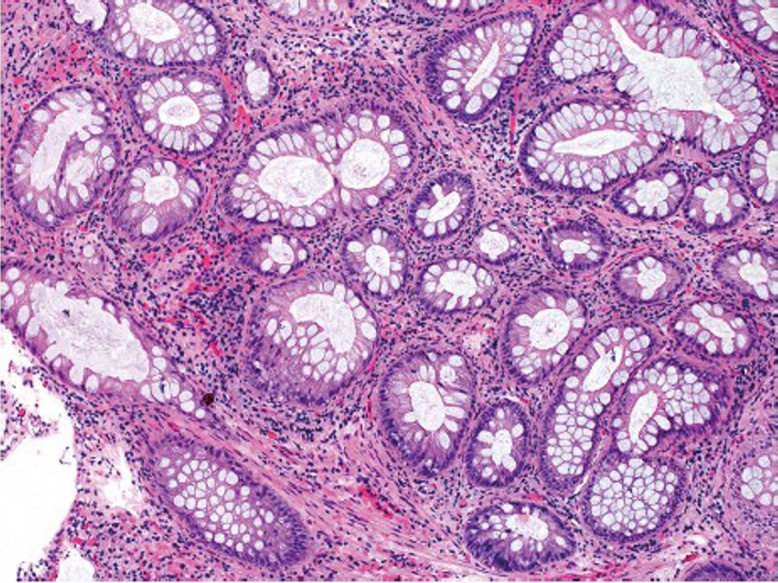
Peutz-Jeghers polyp in the colon. Note the lobular pattern of colonic crypts divided by smooth muscle bundles (original magnification ×100)
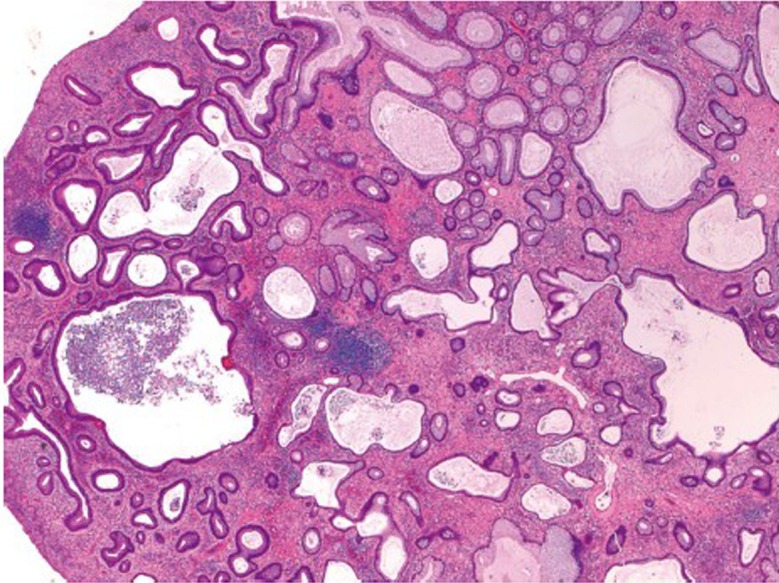
Juvenile polyp showing dilated crypts and inflamed stroma (original magnification ×40)

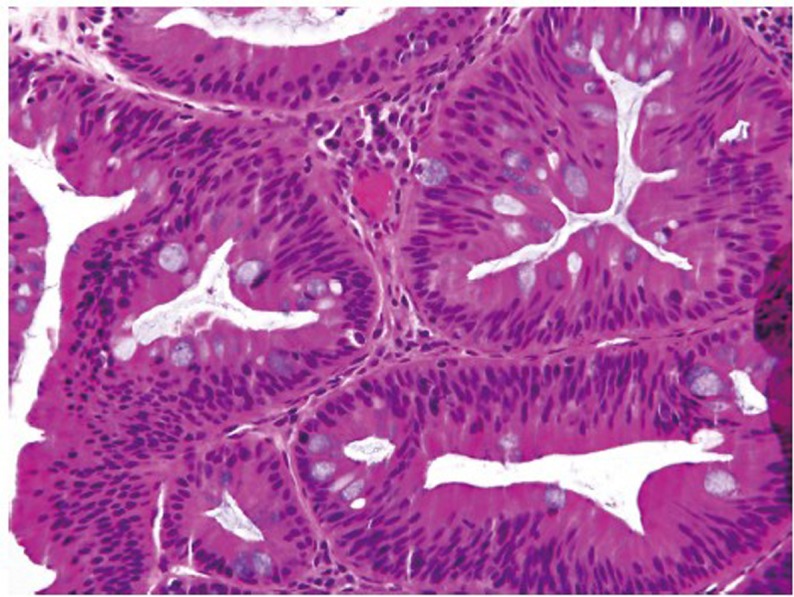
High grade dysplasia showing complex architecture and marked nuclear atypia (original magnification ×400)
A malignant polyp showing adenocarcinomatous glands present within 1 mm of polypectomy margin (original magnification ×100)
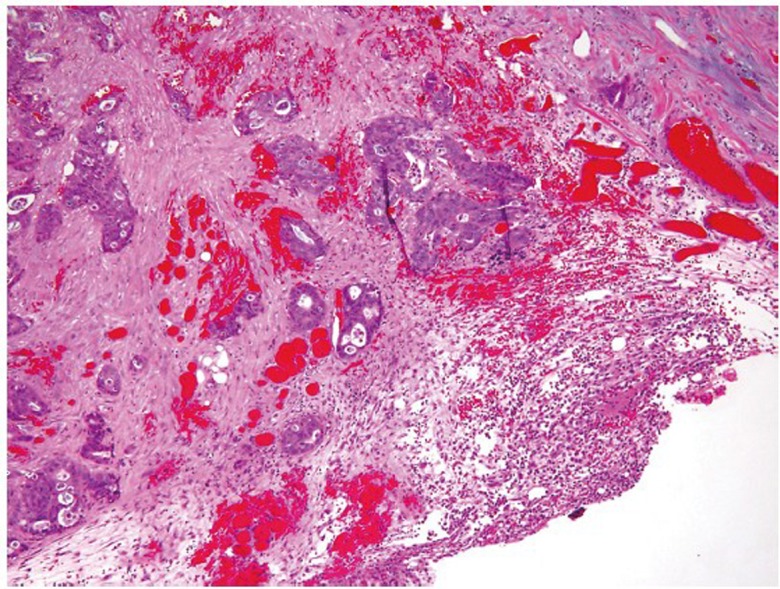
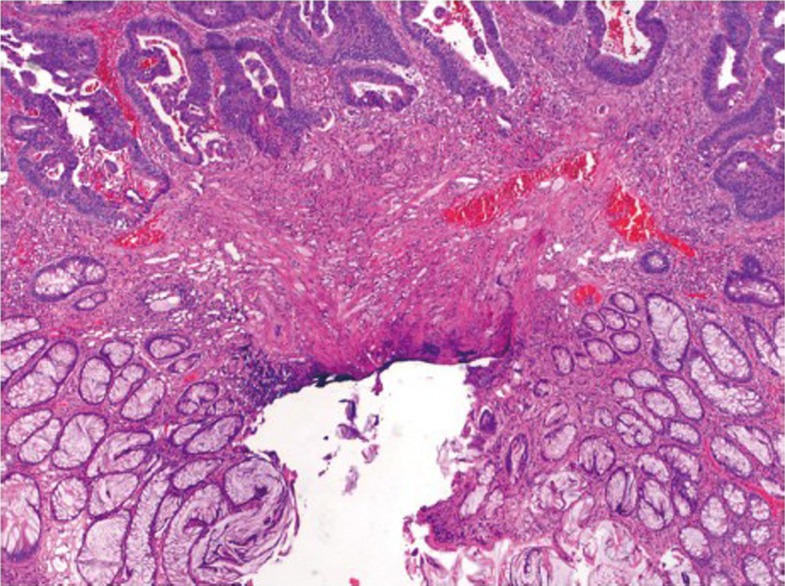
Low power (A. original magnification ×40) and high power (B. original magnification ×200) views of pseudoinvasion in a tubular adenoma. Note the presence of hemorrhage and hemosiderin
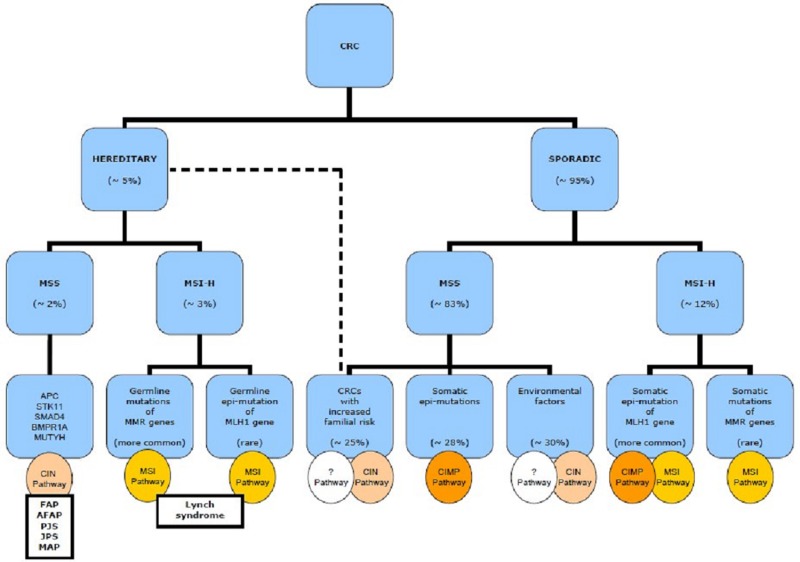
Molecular pathways in colorectal tumorigenesis. CRC, colorectal cancer; MSS, microsatellite stable; MSI-H, high level microsatellite instability; FAP, familial adenomatous polyposis; AFAP, attenuated FAP; PJS, Peutz-Jeghers syndrome; JPS, juvenile polyposis syndrome; MAP, MUTYH-associated polyposis; CIN, chromosomal instability pathway; MSI, microsatellite instability; CIMP, CpG island methylator phenotype; ?, pathways yet undefined
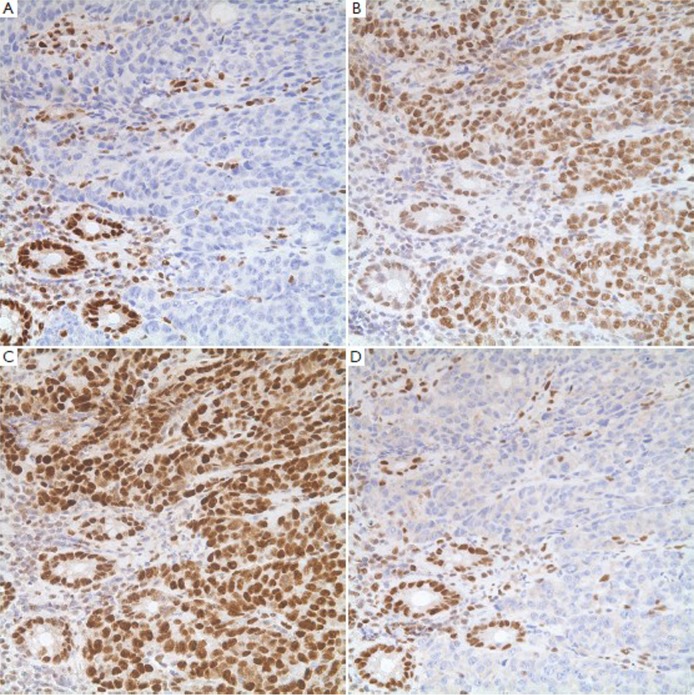
A MSI tumor showing loss of MLH1 (A) and PMS2 (D) protein expression, and normal expression of MSH2 (B) and MSH6 (C). Note the presence of positive staining in benign colonic crypts and inflammatory cells, which serve as good internal controls for the stains (original magnification ×200)
References
-
- Siegel R, Ward E, Brawley O, et al. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 2011;61:212-36 - PubMed
-
- Wang HL, Lopategui J, Amin MB, et al. KRAS mutation testing in human cancers: the pathologist’s role in the era of personalized medicine. Adv Anat Pathol 2010;17:23-32 - PubMed
-
- Hamilton SR, Bosman FT, Boffetta P, et al. Carcinoma of the colon and rectum. In: WHO Classification of Tumours of the Digestive System. Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. Lyon: IARC Press, 2010:134-46.
-
- Compton CC, Fielding LP, Burgart LJ, et al. Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med 2000;124:979-94 - PubMed
-
- Compton CC. Updated protocol for the examination of specimens from patients with carcinomas of the colon and rectum, excluding carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix: a basis for checklists. Cancer Committee. Arch Pathol Lab Med 2000;124:1016-25 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous