

Gastrointestinal lymphomas: Morphology, immunophenotype and molecular features
- PMID: 22943012
- PMCID: PMC3418529
- DOI: 10.3978/j.issn.2078-6891.2012.024
Gastrointestinal lymphomas: Morphology, immunophenotype and molecular features
Abstract
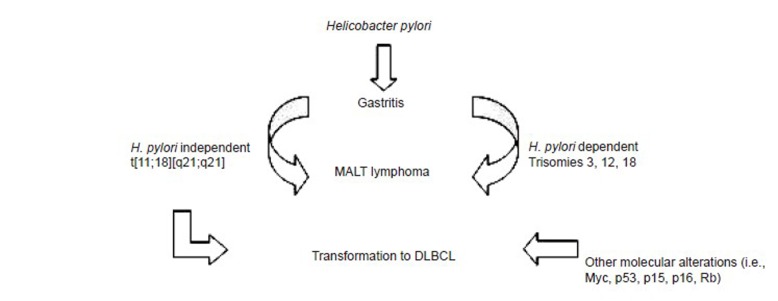
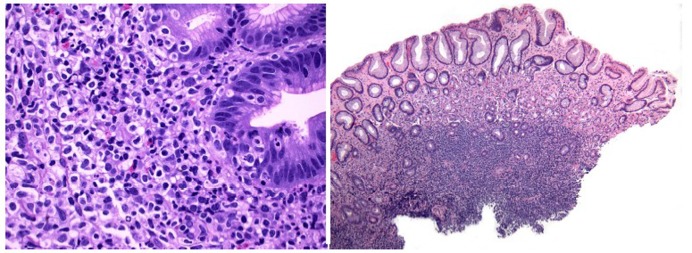
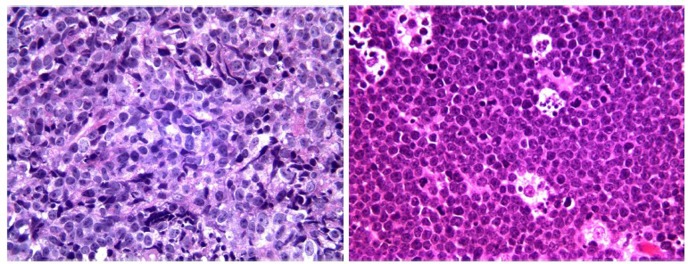
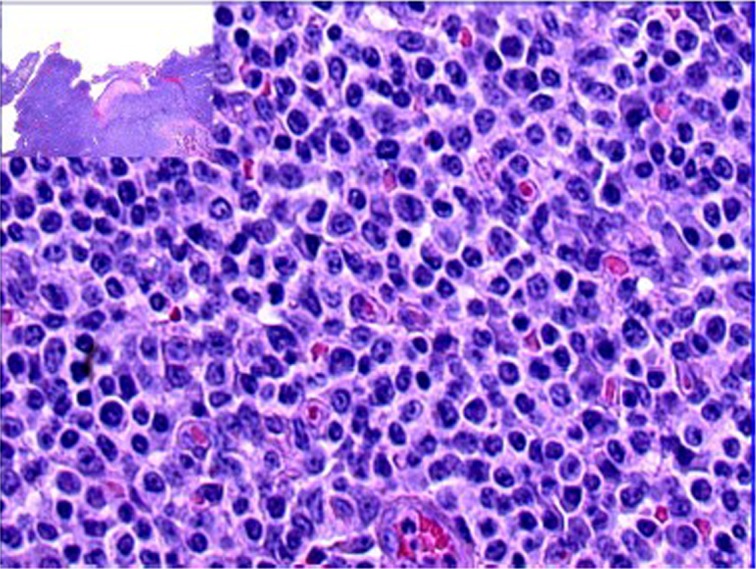
Primary gastrointestinal lymphoma comprises 10-15% of all non-Hodgkin lymphomas and encompasses 30-40% of the total extranodal lymphomas. Approximately 60-75% of cases occur in the stomach, and then the small bowel, ileum, cecum, colon and rectum. Lymphoid neoplasms may consist of mature B, T and less commonly extranodal NK/T cells. Of these, the two most frequently encountered histologic subtypes are extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma), where Helicobacter pylori infection is implicated in a number of cases, and diffuse large B cell lymphoma. Several B cell lymphomas are associated with chromosomal aberrations. Enteropathy-associated T cell lymphoma, type I in particular, usually arises in a background of celiac disease. T cell gene rearrangement confirms clonality. NK/T cell neoplasms are invariably associated with Epstein-Barr virus infection and are often aggressive; thus, differentiation from a benign NK-cell enteropathy is paramount. Although incidence of other hematopoietic malignancies in the gastrointestinal tract such as plasma cell myeloma associated with amyloidosis, plasmablastic lymphoma, Hodgkin disease, histiocytic sarcoma and mast cell sarcoma is extremely rare, these entities have been documented, with the latter two demonstrating aggressive clinical behavior. Endoscopic ultrasonography is an important adjunct in disease staging and follow-up. Conservative antibiotic treatment of stage I MALT lymphomas with associated Helicobacter pylori infection achieves good clinical outcome with high remission rate. Chemotherapy, radiation and rarely surgery are reserved for advanced diseases or cases resistant to conservative therapy and those not associated with Helicobacter pylori infection.
Keywords: Gastrointestinal lymphomas; MALT lymphoma; NK/T-cell enteropathy.
Figures
References
-
- Ferreri AJ, Montalbán C. Primary diffuse large B-cell lymphoma of the stomach. Crit Rev Oncol Hematol 2007;63:65-71 - PubMed
-
- Swerdlow SH, Campo E, Harris NL, et al. Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma). In: Swerdlow SH, Campo E, Harris NL, et al. eds. World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues (4th edition). Lyon:IARC Press, 2008:214-7.
-
- Jezersek Novaković B, Vovk M, Juznic Setina T.A single-center study of treatment outcomes and survival in patients with primary gastric lymphomas between 1990 and 2003. Ann Hematol 2006;85:849-56 - PubMed
LinkOut - more resources
Full Text Sources