

The present state of treatments for articular cartilage defects in the knee
- PMID: 22943326
- PMCID: PMC3954317
- DOI: 10.1308/003588412X13171221592573
The present state of treatments for articular cartilage defects in the knee
Abstract
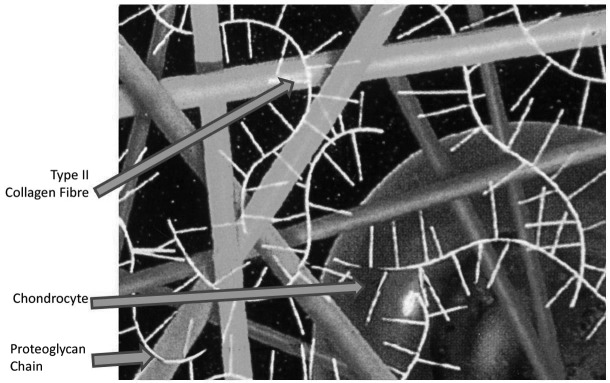
Introduction: Chondral and osteochondral lesions of the knee are notoriously difficult to treat due to the poor healing capacity of articular cartilage and the hostile environment of moving joints, ultimately causing disabling pain and early osteoarthritis. There are many different reconstructive techniques used currently but few are proven to be of value. However, some have been shown to produce a better repair with hyaline-like cartilage rather than fibrocartilage.
Methods: A systematic search of all available online databases including PubMed, MEDLINE(®) and Embase™ was undertaken using several keywords. All the multiple treatment options and methods available were considered. These were summarised, and the evidence for and against them was scrutinised.
Results: A total of 460 articles were identified after cross-referencing the database searches using the keywords. These revealed that autologous and matrix assisted chondrocyte implantation demonstrated both 'good to excellent' histological results and significant improvement in clinical outcomes.
Conclusions: Autologous and matrix assisted chondrocyte implantation have been shown to treat symptomatic lesions successfully with significant histological and clinical improvement. There is, however, still a need for further randomised clinical trials, perfecting the type of scaffold and the use of adjuncts such as growth factors. A list of recommendations for treatment and the potential future trends of managing these lesions are given.
Figures


References
-
- Brown DE, Neumann RD. Orthopaedic Secrets. 3rd edn.Philadelphia, PA: Hanley and Belfus; 2004
-
- Miller MD. Review of Orthopaedics. 5th edn.Philadelphia, PA: Saunders; 2008
-
- Linn FC. Lubrication of animal joints: I. The arthrotripsometer. J Bone Joint Surg Am 1967; 49: 1,079–1,098 - PubMed
-
- Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br 1961; 43: 752–757 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical