

Air leaks following pulmonary resection for lung cancer: is it a patient or surgeon related problem?
- PMID: 22943333
- PMCID: PMC3954324
- DOI: 10.1308/003588412X13171221592258
Air leaks following pulmonary resection for lung cancer: is it a patient or surgeon related problem?
Abstract
Introduction: Prolonged air leak (PAL) is the most common complication after partial lung resection and the most important determinant of length of hospital stay for patients post-operatively. The aim of this study was to determine the risk factors involved in developing air leaks and the consequences of PAL.
Methods: All patients undergoing lung resection between January 2002 and December 2007 in our hospital were studied retrospectively. Univariate analysis to predict risk factors for developing post-operative air leaks included patient demographics, smoking status, pulmonary function tests, disease aetiology (benign, malignant), neoadjuvant therapy (pre-operative radiotherapy/chemotherapy), extent and type of resection, and different consultant surgeons' practice. A logistic regression model was used for multivariate analysis.
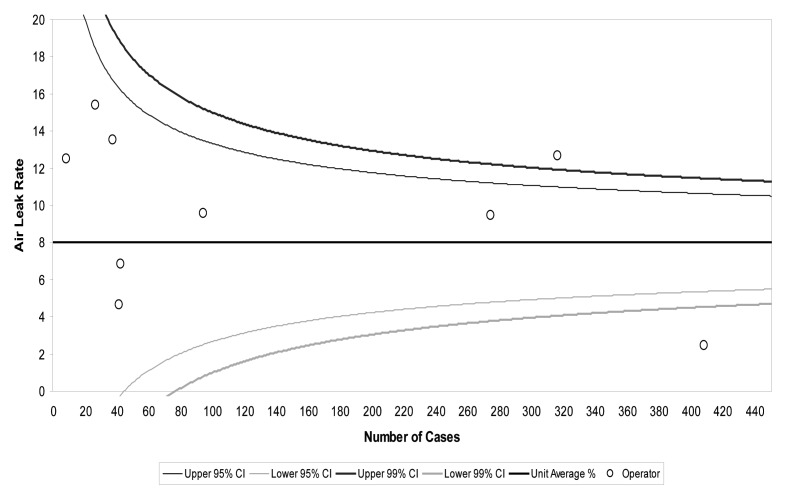
Results: A total of 1,911 lung resections were performed over the 6-year study period. An air leak lasting more than 6 days post-operatively was present in 129 patients (6.7%). This included 100 out of the 1,250 patients (8%) from the lobectomy group and 29 out of the 661 patients (4.4%) from the wedge/segmentectomy group. Using the multivariate analysis, the risk factors for developing an air leak included a low predicted forced expiratory volume in 1 second (pFEV(1)) (p<0.001), performing an upper lobectomy (p=0.002) and different consultant practice (p=0.02). PAL was associated with increased length of stay (p<0.0001), in-hospital mortality (p=0.003) and intensive care unit readmission (p=0.05).
Conclusions: Air leaks after pulmonary resections were at an acceptable rate in our series. Particular patients are at a higher risk but meticulous surgical technique is vital in reducing their incidence. Our study shows that pFEV1 is the strongest predictor of post-operative air leaks.
Figures
References
-
- Stéphan F, Boucheseiche S, Hollande Jet al.Pulmonary complications following lung resection: a comprehensive analysis of incidence and possible risk factors.Chest 2000; 118: 1,263–1,270 - PubMed
-
- Adebonojo SA.How prolonged is ‘prolonged air leak’? Ann Thorac Surg 1995; 59: 549–550 - PubMed
-
- Brunelli A, Xiume F, Al Refai Met al.Air leaks after lobectomy increase the risk of empyema but not of cardiopulmonary complications: a case-matched analysis. Chest 2006; 130: 1,150–1,156 - PubMed
-
- Varela G, Jiménez MF, Novoa N, Aranda JL. Estimating hospital costs attributable to prolonged air leak in pulmonary lobectomy. Eur J Cardiothorac Surg 2005; 27: 329–333 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical