

Efficacy of a systematic depression management program in high utilizers of primary care: a randomized trial
- PMID: 22943609
- PMCID: PMC3489593
- DOI: 10.1186/1472-6963-12-298
Efficacy of a systematic depression management program in high utilizers of primary care: a randomized trial
Abstract
Background: Approximately 25% of so-called high utilizers of medical care are estimated to suffer from depression. A large proportion of these individuals remain undiagnosed and untreated. This study aims to examine the effects of a systematic screening and collaborative treatment program on depression severity in small primary care practices of the German outpatient health care system.
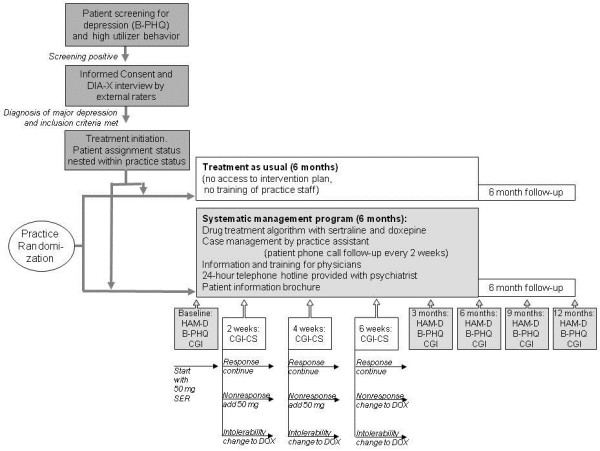
Method: High utilizers of primary care who screened positive for depressive symptoms on the Brief Psychiatric Health Questionnaire (B-PHQ) were further diagnosed using the DIA-X, a standardized diagnostic interview, performed by trained and supervised interviewers. Patients with major depression were randomized (cluster randomization by practice) to (a) a six-month treatment program of pharmacotherapy, standardized patient and provider education, and physician and patient counseling or (b) six months of usual medical care. All subjects were followed for a 12-month observation period using the 17-item Hamilton Depression Rating scale (HAMD-17) rated by the treating physicians and the B-PHQ-9 rated by the patients.
Results: A total of 63 high utilizer patients were included in the trial (17 male, 46 female), 19 randomized to intervention, 44 to usual care. The mean age was 49.7 (SD 13.8). Most patients had one or more somatic co-morbidities. There was no significant difference in response (defined as a decrease in the HAMD-17 sum score of at least 50%) after six months of treatment (50% vs. 42%, p = 0.961, all analyses adjusted for age) and after 12 months of treatment (83% vs. 54%, p = 0.282) between groups. Using patient self-rating assessments with the B-PHQ-9 questionnaire the intervention was superior to treatment as usual at six months (83% vs. 16%, p = 0.000).There was no significant difference in HAMD-17 depression severity at six months between the groups (10.5 (SD 7.6) vs. 12.3 (SD 7.8), p = 0.718), but a trend at 12 months (4.7 (SD 8.0) vs. 11.2 (SD 7.4), p = 0.083). Again, using B-PHQ-9 sum scores depression severity was significantly lower in the intervention group than in the treatment as usual group after six months (6.4 (SD 5.2) vs. 11.5 (SD 5.8), p = 0.020), but not at 12 months (7.9 (SD 8.7) vs. 9.0 (SD 5.2), p = 0.858).
Conclusion: A systematic collaborating treatment program for depression in high utilizers in primary care showed superiority to treatment as usual only in terms of patients' self-assessment but not according to physicians' assessment. The advance of the intervention group at 6 months was lost after 12 months of follow-up. Overall, positive results from similar trials in the US health care systems could not be confirmed in a German primary care setting.
Figures
References
-
- Bromet E, Andrade LH, Hwang I, Sampson NA, Alonso J, de Girolamo G, de Graaf R, Demyttenaere K, Hu C, Iwata N, Karam AN, Kaur J, Kostyuchenko S, Lépine JP, Levinson D, Matschinger H, Mora ME, Browne MO, Posada-Villa J, Viana MC, Williams DR, Kessler RC. Cross-national epidemiology of DSM-IV major depressive episode. BMC Medicine. 2011;9:90. doi: 10.1186/1741-7015-9-90. - DOI - PMC - PubMed
-
- The ESEMeD/MHEDEA 2000 Investigators. Prevalence of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand. 2004;109(suppl. 420):21–27. - PubMed
-
- Jacobi F, Wittchen HU, Hölting C, Höfler M, Pfister H, Müller N, Lieb R. Prevalence, co-morbidity and correlates of mental disorders in the general population: results from the German Health Interview and Examination Survey (GHS) Psychol Med. 2004;34:597–611. doi: 10.1017/S0033291703001399. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
