

Surgery in a population-based cohort of Crohn's disease from Olmsted County, Minnesota (1970-2004)
- PMID: 22945286
- PMCID: PMC3572861
- DOI: 10.1038/ajg.2012.298
Surgery in a population-based cohort of Crohn's disease from Olmsted County, Minnesota (1970-2004)
Abstract
Objectives: We sought to estimate the need for surgery in an American population-based cohort of Crohn's disease.
Methods: The medical records of 310 incident cases of Crohn's disease from Olmsted County, Minnesota, diagnosed between 1970 and 2004, were reviewed through March 2009. Cumulative incidence was estimated using the Kaplan-Meier method, and associations between baseline factors and time to first event were assessed using proportional hazards regression and expressed as hazards ratios (HRs) with 95% confidence intervals.
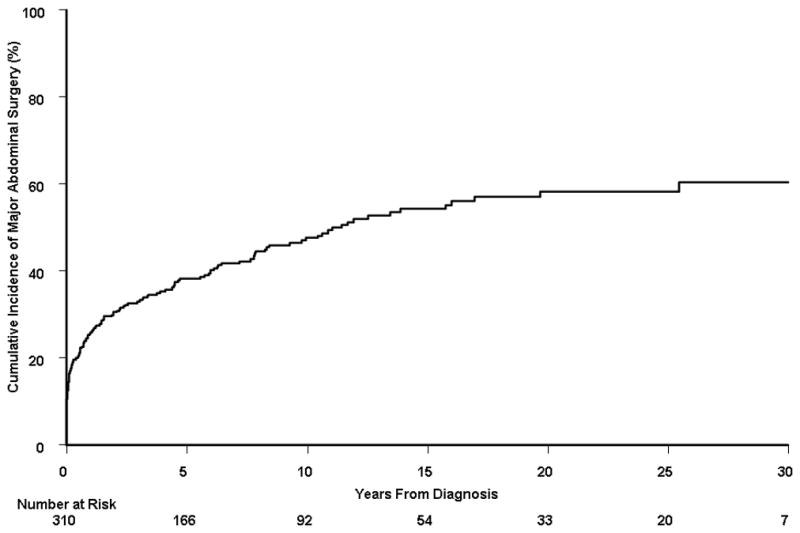
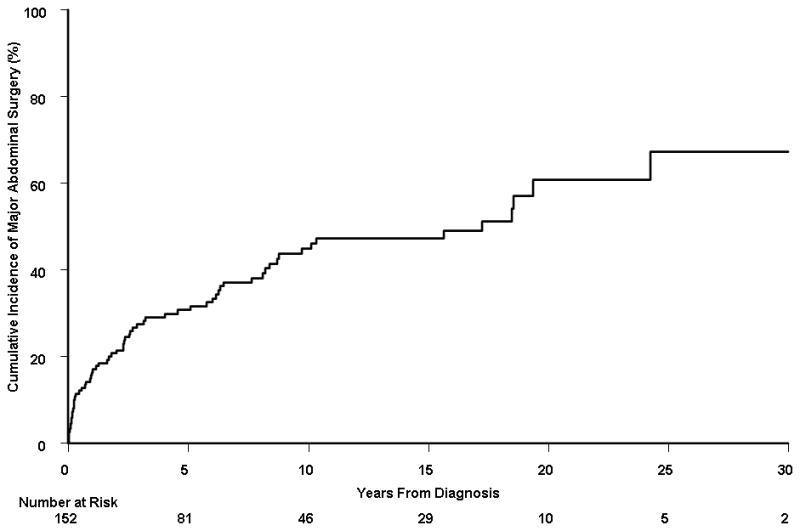
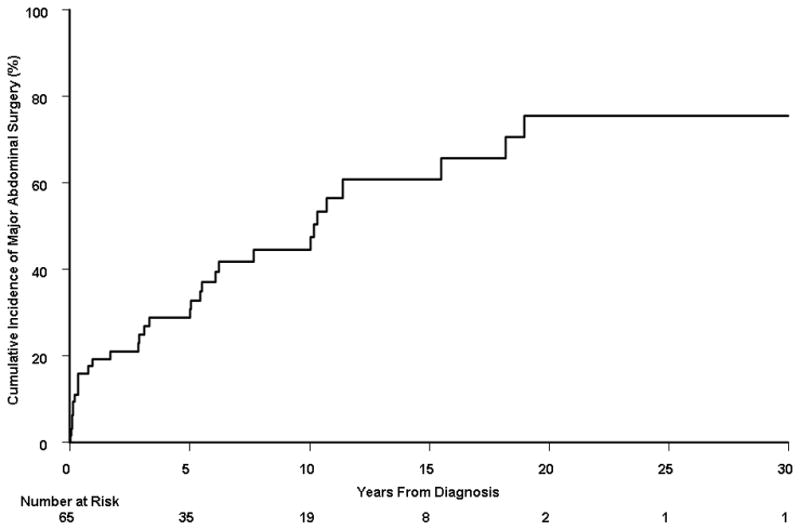
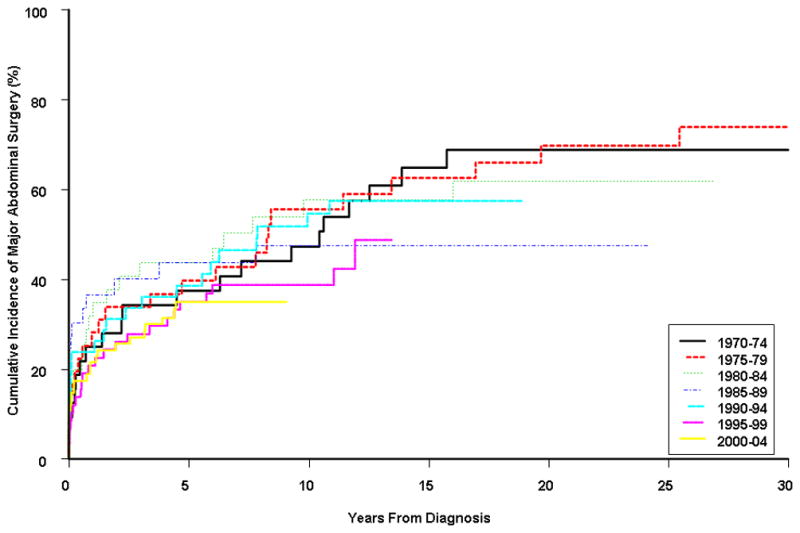
Results: Median follow-up per patient was 12 years. One hundred and fifty-two patients underwent at least 1 major abdominal surgery, 65 had at least 2 surgeries, and 32 had at least 3 surgeries. The cumulative probability of major abdominal surgery was 38, 48, and 58% at 5, 10, and 20 years after diagnosis, respectively. Baseline factors significantly associated with time to major abdominal surgery were: ileocolonic (HR, 3.3), small bowel (HR, 3.4), and upper gastrointestinal (HR, 4.0) extent, relative to colonic alone; current cigarette smoking (HR, 1.7), male gender (HR, 1.6), penetrating disease behavior (HR, 2.7), and early corticosteroid use (HR=1.6). Major abdominal surgery rates remained stable, with 5-year cumulative probabilities in 1970-1974 and 2000-2004 of 37.5 and 35.1%, respectively.
Conclusions: The cumulative probability of major abdominal surgery in this population-based cohort of Crohn's disease approached 60% after 20 years of disease, and many patients required second or third surgeries. Non-colonic disease extent, current smoking, male gender, penetrating disease behavior, and early steroid use were significantly associated with major abdominal surgery.
Conflict of interest statement
Figures
References
-
- Peyrin-Biroulet L, Loftus EV, Jr, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105:289–97. - PubMed
-
- Bougen G, Peyrin-Biroulet L. Surgery for Adult Crohn’s Disease: What is the Actual Risk? Gut. 2011;60:1178–81. - PubMed
-
- Nguyen GC, Nugent Z, Shaw S, Bernstein CN. Outcomes of patients with Crohn’s disease improved from 1988 to 2008 and were associated with increased specialist care. Gastroenterology. 2011;141:90–7. - PubMed
-
- Munkholm P, Langholz E, Davidsen M, Binder V. Intestinal cancer risk and mortality in patients with Crohn’s disease. Gastroenterology. 1993;105:1716–23. - PubMed
-
- Solberg IC, Vatn MH, Hoie O, Stray N, Sauar J, Jahnsen J, Moum B, Lygren I. Clinical course in Crohn’s disease: results of a Norwegian population-based ten-year follow-up study. Clin Gastroenterol Hepatol. 2007;5:1430–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
