

The genetics of hyperuricaemia and gout
- PMID: 22945592
- PMCID: PMC3645862
- DOI: 10.1038/nrrheum.2012.144
The genetics of hyperuricaemia and gout
Abstract
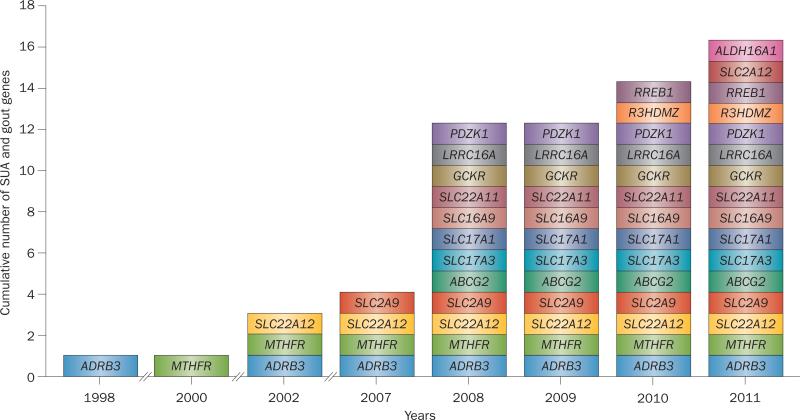
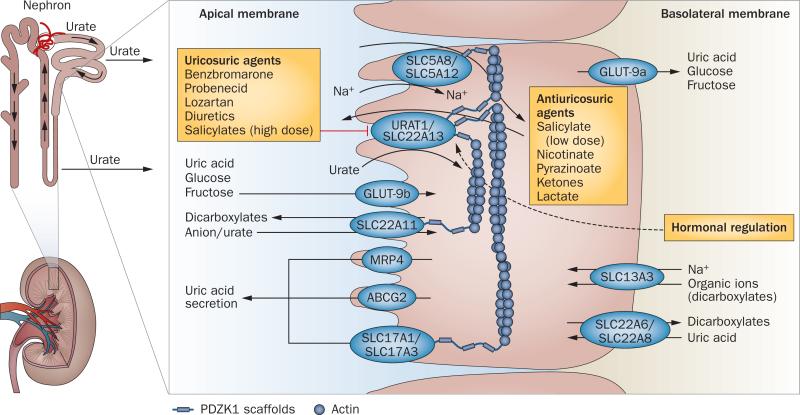
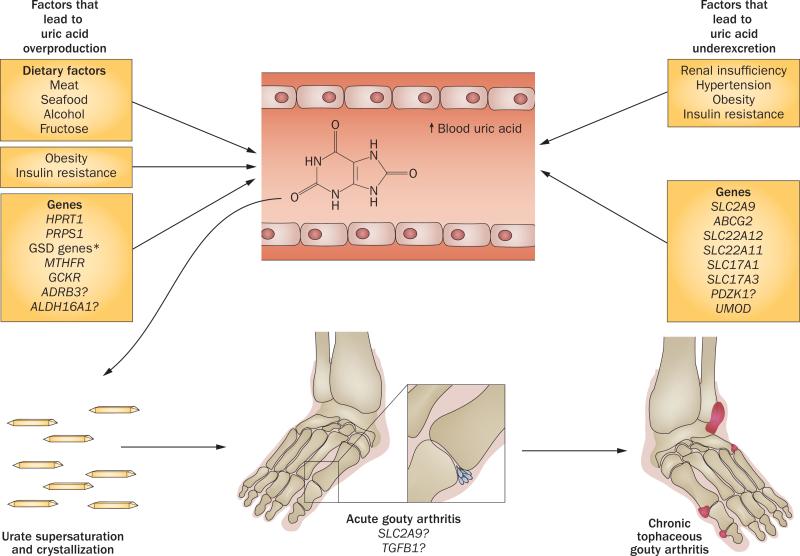
Gout is a common and very painful inflammatory arthritis caused by hyperuricaemia. This review provides an update on the genetics of hyperuricaemia and gout, including findings from genome-wide association studies. Most of the genes that associated with serum uric acid levels or gout are involved in the renal urate-transport system. For example, the urate transporter genes SLC2A9, ABCG2 and SLC22A12 modulate serum uric acid levels and gout risk. The net balance between renal urate absorption and secretion is a major determinant of serum uric acid concentration and loss-of-function mutations in SLC2A9 and SLC22A12 cause hereditary hypouricaemia due to reduced urate absorption and unopposed urate secretion. However, the variance in serum uric acid explained by genetic variants is small and their clinical utility for gout risk prediction seems limited because serum uric acid levels effectively predict gout risk. Urate-associated genes and genetically determined serum uric acid levels were largely unassociated with cardiovascular-metabolic outcomes, challenging the hypothesis of a causal role of serum uric acid in the development of cardiovascular disease. Strong pharmacogenetic associations between HLA-B*5801 alleles and severe allopurinol-hypersensitivity reactions were shown in Asian and European populations. Genetic testing for HLA-B*5801 alleles could be used to predict these potentially fatal adverse effects.
Figures
References
-
- Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and hyperuricaemia in the US general population: The National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011;63:3136–3141. - PubMed
-
- Choi HK, Mount DB, Reginato AM, American College of Physicians & American Physiological Society Pathogenesis of gout. Ann. Intern. Med. 2005;143:499–516. - PubMed
-
- Choi HK, Ford ES, Li C, Curhan G. Prevalence of the metabolic syndrome in patients with gout: the Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2007;57:109–115. - PubMed
-
- Abbott RD, Brand FN, Kannel WB, Castelli WP. Gout and coronary heart disease: the Framingham Study. J. Clin. Epidemiol. 1988;41:237–242. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
