

Reducing salt intake for prevention of cardiovascular diseases in high-risk patients by advanced health education intervention (RESIP-CVD study), Northern Thailand: study protocol for a cluster randomized trial
- PMID: 22947342
- PMCID: PMC3533738
- DOI: 10.1186/1745-6215-13-158
Reducing salt intake for prevention of cardiovascular diseases in high-risk patients by advanced health education intervention (RESIP-CVD study), Northern Thailand: study protocol for a cluster randomized trial
Abstract
Background: Decreasing salt consumption can prevent cardiovascular diseases (CVD). Practically, it is difficult to promote people's awareness of daily salt intake and to change their eating habits in terms of reducing salt intake for better cardiovascular health. Health education programs visualizing daily dietary salt content and intake may promote lifestyle changes in patients at high risk of cardiovascular diseases.
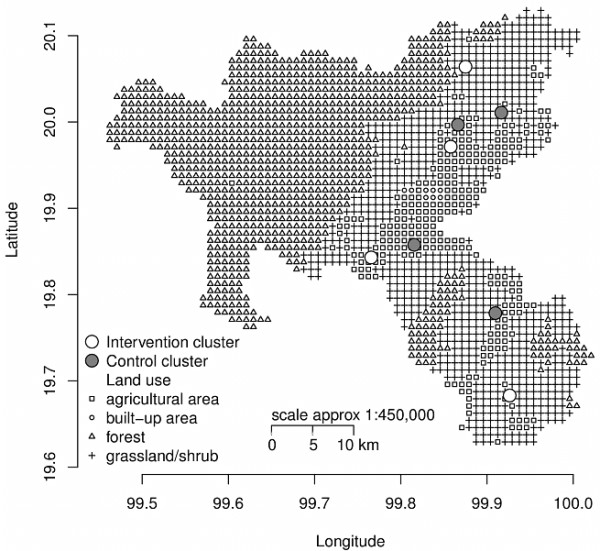
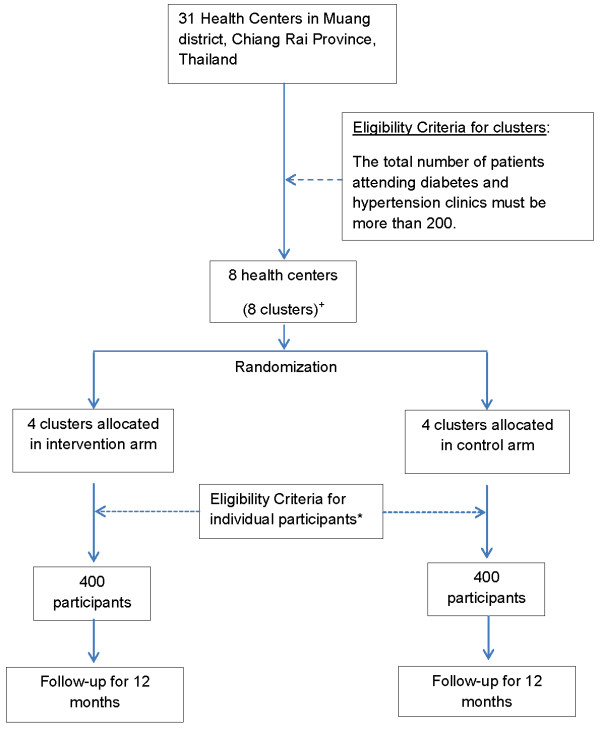
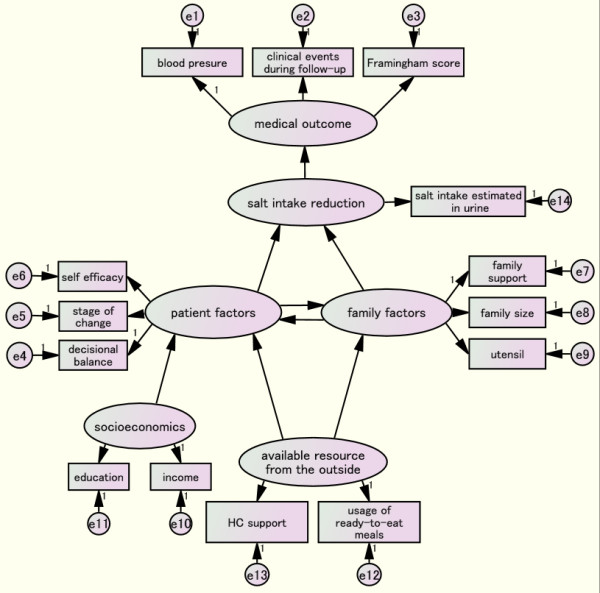
Methods/design: This is a cluster randomized trial. A total of 800 high-CVD-risk patients attending diabetes and hypertension clinics at health centers in Muang District, Chiang Rai province, Thailand, will be studied with informed consent. A health center recruiting 100 participants is a cluster, the unit of randomization. Eight clusters will be randomized into intervention and control arms and followed up for 1 year. Within the intervention clusters the following will be undertaken: (1) salt content in the daily diet will be measured and shown to study participants; (2) 24-hour salt intake will be estimated in overnight-collected urine and the results shown to the participants; (3) a dietician will assist small group health education classes in cooking meals with less salt. The primary outcome is blood pressure change at the 1-year follow-up. Secondary outcomes at the 1-year follow-up are estimated 24-hoursalt intake, incidence of CVD events and CVD death. The intention-to-treat analysis will be followed.Blood pressure and estimated 24-hour salt intake will be compared between intervention and control groups at the cluster and individual level at the 1-year follow-up. Clinical CVD events and deaths will be analyzed by time-event analysis. Retinal blood vessel calibers of CVD-risk patients will be assessed cross-sectionally. Behavioral change to reduce salt intake and the influencing factors will be determined by structured equation model (SEM). Multilevel regression analyses will be applied. Finally, the cost effectiveness of the intervention will be analyzed.
Discussion: This study is unique as it will recruit the individuals most vulnerable to CVD morbidity and mortality by applying the general Framingham CVD risk scoring system. Dietary salt reduction will be applied as a prioritized, community level intervention for the prevention of CVD in a developing country.
Trial registration: ISRCTN39416277.
Figures

References
-
- Cardiovascular diseases. Key messages to protect heart health. http://www.who.int/cardiovascular_diseases/en/
-
- Bureau of Health Policy and Strategy, Ministry of Public Health Thailand. Number of Deaths and Death Rates per 100,000 Population by Leading Causes of Death. 2005–2009. http://bps.ops.moph.go.th/Statistic/2.3.4-52.pdf.
-
- Bureau of Health Policy and Strategy, Ministry of Public Health Thailand. The top ten causes of morbidity rate per 100,000 population in the inpatients. 2009. http://bps.ops.moph.go.th/Ill/%E0%B8%9B%E0%B9%88%E0%B8%A7%E0%B8%A252/10%....
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
