

Clinical features of bladder cancer in primary care
- PMID: 22947580
- PMCID: PMC3426598
- DOI: 10.3399/bjgp12X654560
Clinical features of bladder cancer in primary care
Erratum in
- Br J Gen Pract. 2014 Mar;64(620):126
Abstract
Background: Bladder cancer accounts for over 150,000 deaths worldwide. No screening is available, so diagnosis depends on investigations of symptoms. Of these, only visible haematuria has been studied in primary care.
Aim: To identify and quantify the features of bladder cancer in primary care.
Design and setting: Case-control study, using electronic medical records from UK primary care.
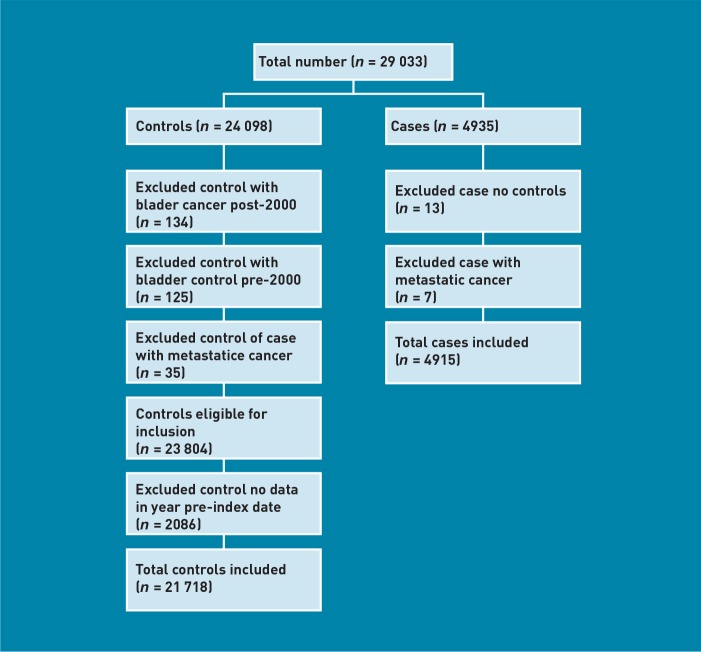
Method: Participants were 4915 patients aged ≥40 years, diagnosed with bladder cancer January 2000 to December 2009, and 21,718 age, sex, and practice-matched controls, were selected from the General Practice Research Database, UK. All clinical features independently associated with bladder cancer using conditional logistic regression were identified, and their positive predictive values for bladder cancer, singly and in combination, were estimated.
Results: Cases consulted their GP more frequently than controls before diagnosis: median 15 consultations (interquartile range 9-22) versus 8 (4-15): P<0.001. Seven features were independently associated with bladder cancer: visible haematuria, odds ratio 34 (95% confidence interval [CI] = 29 to 41), dysuria 4.1 (95% CI = 3.4 to 5.0), urinary tract infection 2.2 (95% CI = 2.0 to 2.5), raised white blood cell count 2.1 (95% CI = 1.6 to 2.8), abdominal pain 2.0 (95% CI = 1.6 to 2.4), constipation 1.5 (95% CI = 1.2 to 1.9), raised inflammatory markers 1.5 (95% CI = 1.2 to 1.9), and raised creatinine 1.3 (95% CI = 1.2 to 1.4). The positive predictive value for visible haematuria in patients aged ≥60 years was PPV of 2.6% (95% CI = 2.2 to 3.2).
Conclusion: Visible haematuria is the commonest and most powerful predictor of bladder cancer in primary care, and warrants investigation. Most other previously reported features of bladder cancer were associated with the disease, but with low predictive values. There is a need for improved diagnostic methods, for those patients whose bladder cancer presents without visible haematuria.
Figures

Comment in
-
Predicting risk of bladder cancer in the UK.Br J Gen Pract. 2012 Nov;62(604):570-1. doi: 10.3399/bjgp12X658160. Br J Gen Pract. 2012. PMID: 23211155 Free PMC article. No abstract available.
References
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. - PubMed
-
- Mowatt G, Zhu S, Kilonzo M, et al. Systematic review of the clinical effectiveness and cost-effectiveness of photodynamic diagnosis and urine biomarkers (FISH, ImmunoCyt, NMP22) and cytology for the detection and follow-up of bladder cancer. Health Technol Assess. 2010;14(4):1–131. - PubMed
-
- National Audit Office. Delivering the cancer reform strategy. London: The Stationery Office; 2010.
-
- Wallace D, Bryan R, Dunn J, et al. Delay and survival in bladder cancer. BJU Int. 2002;89(9):868–878. - PubMed
-
- Liedberg F, Anderson H, Mansson A, Mansson W. Diagnostic delay and prognosis in invasive bladder cancer. Scand J Urol Nephrol. 2003;37(5):396–400. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical