

Accuracy of symptoms, signs, and C-reactive protein for early chronic obstructive pulmonary disease
- PMID: 22947584
- PMCID: PMC3426602
- DOI: 10.3399/bjgp12X654605
Accuracy of symptoms, signs, and C-reactive protein for early chronic obstructive pulmonary disease
Abstract
Background: Guidelines recommend detection of early chronic obstructive pulmonary disease (COPD), but evidence on the diagnostic work-up for COPD only concerns advanced and established COPD.
Aim: To quantify the accuracy of symptoms and signs for early COPD, and the added value of C-reactive protein (CRP), in primary care patients presenting with cough.
Design and setting: Cross-sectional diagnostic study of 73 primary care practices in the Netherlands.
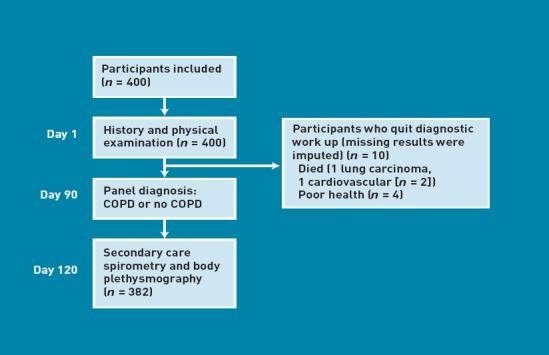
Method: Four hundred primary care patients (182 males, mean age 63 years) older than 50 years, presenting with persistent cough (>14 days) without established COPD participated, of whom 382 completed the study. They underwent a systematic diagnostic work-up of symptoms, signs, conventional laboratory CRP level, and hospital lung functions tests, including body plethysmography, and an expert panel decided whether COPD was present (reference test). The independent value of all items was estimated by multivariable logistic regression analysis.
Results: According to the expert panel, 118 patients had COPD (30%). Symptoms and signs with independent diagnostic value were age, sex, current smoking, smoking more than 20 pack-years, cardiovascular comorbidity, wheezing complaints, diminished breath sounds, and wheezing on auscultation. Combining these items resulted in an area under the receiver operating characteristic curve (ROC area) of 0.79 (95% confidence interval = 0.74 to 0.83) after internal validation. The proportion of subjects with elevated CRP was higher in those with early COPD, but CRP added no relevant diagnostic information above symptoms and signs.
Conclusion: In subjects presenting with persistent cough, the CRP level has no added value for detection of early COPD.
Similar articles
-
Should chest examination be reinstated in the early diagnosis of chronic obstructive pulmonary disease?Int J Chron Obstruct Pulmon Dis. 2013;8:369-77. doi: 10.2147/COPD.S47992. Epub 2013 Jul 31. Int J Chron Obstruct Pulmon Dis. 2013. PMID: 23983462 Free PMC article.
-
Use of serum C reactive protein and procalcitonin concentrations in addition to symptoms and signs to predict pneumonia in patients presenting to primary care with acute cough: diagnostic study.BMJ. 2013 Apr 30;346:f2450. doi: 10.1136/bmj.f2450. BMJ. 2013. PMID: 23633005 Free PMC article. Clinical Trial.
-
Accuracy of history, wheezing, and forced expiratory time in the diagnosis of chronic obstructive pulmonary disease.J Gen Intern Med. 2002 Sep;17(9):684-8. doi: 10.1046/j.1525-1497.2002.20102.x. J Gen Intern Med. 2002. PMID: 12220364 Free PMC article.
-
Diagnostic management of chronic obstructive pulmonary disease.Neth J Med. 2012 Jan;70(1):6-11. Neth J Med. 2012. PMID: 22271808 Review.
-
The diagnostic value of history and physical examination for COPD in suspected or known cases: a systematic review.Fam Pract. 2009 Aug;26(4):260-8. doi: 10.1093/fampra/cmp026. Epub 2009 May 7. Fam Pract. 2009. PMID: 19423699
Cited by
-
Should chest examination be reinstated in the early diagnosis of chronic obstructive pulmonary disease?Int J Chron Obstruct Pulmon Dis. 2013;8:369-77. doi: 10.2147/COPD.S47992. Epub 2013 Jul 31. Int J Chron Obstruct Pulmon Dis. 2013. PMID: 23983462 Free PMC article.
-
Weighing the evidence for pharmacological treatment interventions in mild COPD; a narrative perspective.Respir Res. 2019 Jul 8;20(1):141. doi: 10.1186/s12931-019-1108-9. Respir Res. 2019. PMID: 31286970 Free PMC article. Review.
-
Drop in lung function during asthma and COPD exacerbations - can it be assessed without spirometry?Int J Chron Obstruct Pulmon Dis. 2016 Dec 8;11:3145-3152. doi: 10.2147/COPD.S123315. eCollection 2016. Int J Chron Obstruct Pulmon Dis. 2016. PMID: 27994453 Free PMC article.
-
Guidelines for diagnosis and management of chronic obstructive pulmonary disease: Joint ICS/NCCP (I) recommendations.Lung India. 2013 Jul;30(3):228-67. doi: 10.4103/0970-2113.116248. Lung India. 2013. PMID: 24049265 Free PMC article.
-
Laryngeal measurements and diagnostic tools for diagnosis of chronic obstructive pulmonary disease.Ann Fam Med. 2015 Jan-Feb;13(1):49-52. doi: 10.1370/afm.1733. Ann Fam Med. 2015. PMID: 25583892 Free PMC article.
References
-
- Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. - PubMed
-
- Bednarek M, Maciejewski J, Wozniak M, et al. Prevalence, severity and underdiagnosis of COPD in the primary care setting. Thorax. 2008;63(5):402–407. - PubMed
-
- Holleman DR, Jr, Simel DL. Does the clinical examination predict airflow limitation? JAMA. 1995;273(4):313–319. - PubMed
-
- McAlister FA, Straus SE, Sackett DL. Why we need large, simple studies of the clinical examination: the problem and a proposed solution. CARE-COAD1 group. Clinical Assessment of the Reliability of the Examination-Chronic Obstructive Airways Disease Group. Lancet. 1999;354(9191):1721–1724. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous