

Propagation of uncertainty in Bayesian diagnostic test interpretation
- PMID: 22948322
- PMCID: PMC6785978
- DOI: 10.1097/SMJ.0b013e3182621a2c
Propagation of uncertainty in Bayesian diagnostic test interpretation
Abstract
Objectives: Bayesian interpretation of diagnostic test results usually involves point estimates of the pretest probability and the likelihood ratio corresponding to the test result; however, it may be more appropriate in clinical situations to consider instead a range of possible values to express uncertainty in the estimates of these parameters. We thus sought to demonstrate how uncertainty in sensitivity, specificity, and disease pretest probability can be accommodated in Bayesian interpretation of diagnostic testing.
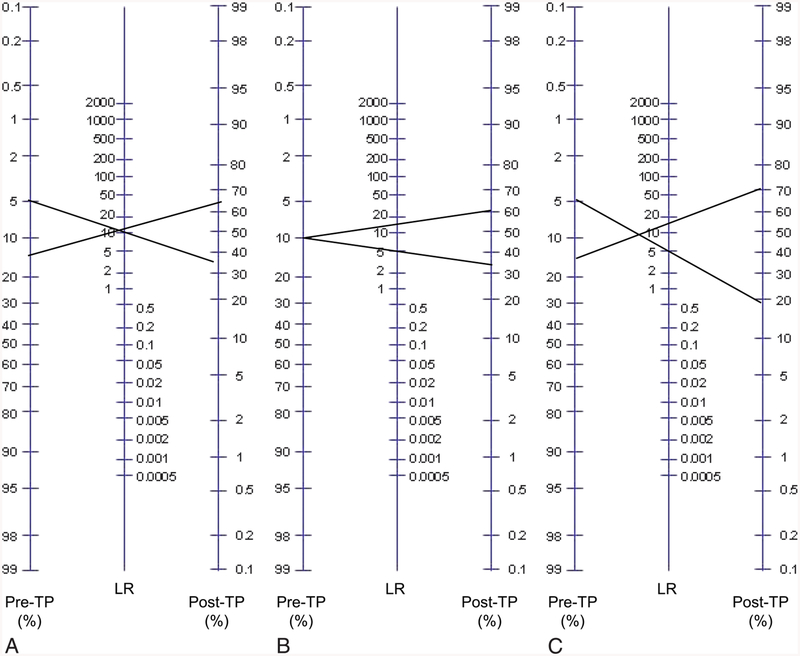
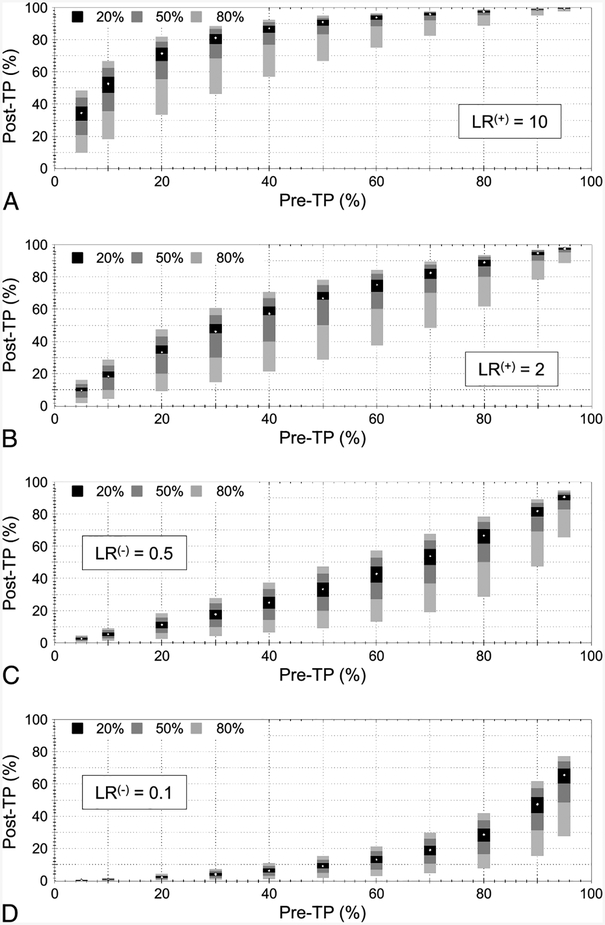
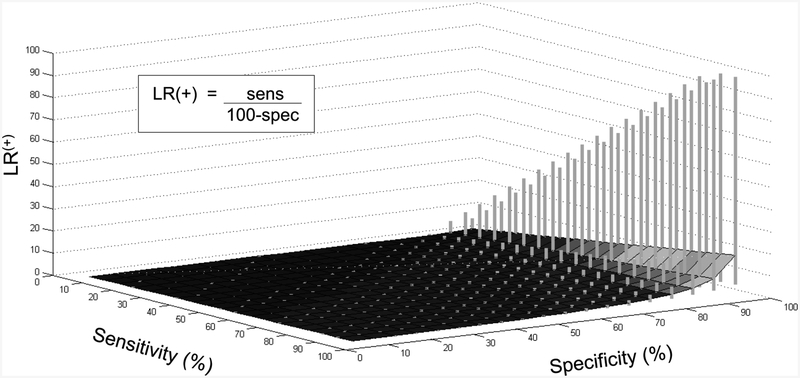
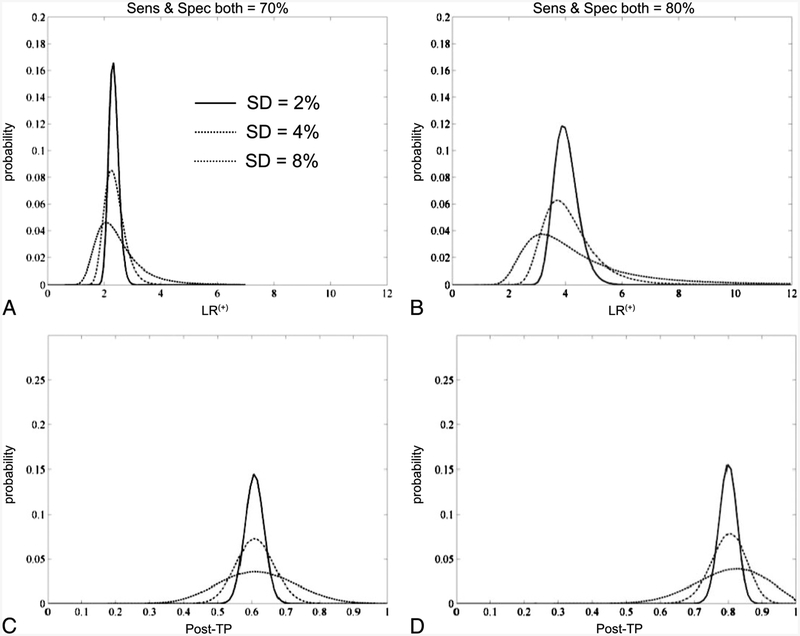
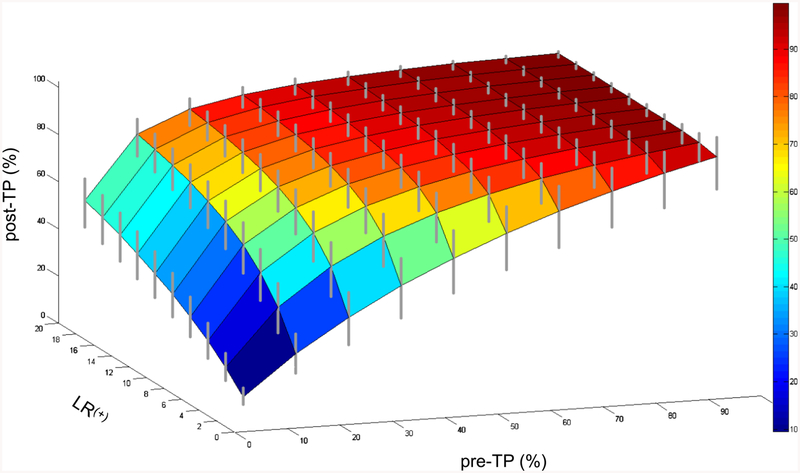
Methods: We investigated three questions: How does uncertainty in the likelihood ratio propagate to the posttest probability range, assuming a point estimate of pretest probability? How does uncertainty in the sensitivity and specificity of a test affect uncertainty in the likelihood ratio? How does uncertainty propagate when present in both the pretest probability and the likelihood ratio?
Results: Propagation of likelihood ratio uncertainty depends on the pretest probability and is more prominent for unexpected test results. Uncertainty in sensitivity and specificity propagates into the calculation of likelihood ratio prominently as these parameters approach 100%; even modest errors of ± 10% caused dramatic propagation. Combining errors of ± 20% in the pretest probability and in the likelihood ratio exhibited modest propagation to posttest probability, suggesting a realistic target range for clinical estimations.
Conclusions: The results provide a framework for incorporating ranges of uncertainty into Bayesian reasoning. Although point estimates simplify the implementation of Bayesian reasoning, it is important to recognize the implications of error propagation when ranges are considered in this multistep process.
Figures
Comment in
-
Commentary on "propagation of uncertainty in bayesian diagnostic test interpretation".South Med J. 2012 Sep;105(9):460-1. doi: 10.1097/SMJ.0b013e3182621b1a. South Med J. 2012. PMID: 22948323 No abstract available.
References
-
- Gallagher EJ. Clinical utility of likelihood ratios. Ann Emerg Med 1998;31:391–397. - PubMed
-
- Halkin A, Reichman J, Schwaber M, et al. Likelihood ratios: getting diagnostic testing into perspective. Q J Med 1998;91:247–258. - PubMed
-
- Dolan JG, Bordley DR, Mushlin AI. An evaluation of clinicians’ subjective prior probability estimates. Med Decis Making 1986; 6: 216–223. - PubMed
-
- Lyman GH, Balducci L. Overestimation of test effects in clinical judgment. J Cancer Educ 1993;8:297–307. - PubMed
-
- Lyman GH, Balducci L. The effect of changing disease risk on clinical reasoning. J Gen Intern Med 1994;9:488–495. - PubMed