

Prevalence and prognosis of unrecognized myocardial infarction determined by cardiac magnetic resonance in older adults
- PMID: 22948699
- PMCID: PMC4137910
- DOI: 10.1001/2012.jama.11089
Prevalence and prognosis of unrecognized myocardial infarction determined by cardiac magnetic resonance in older adults
Abstract
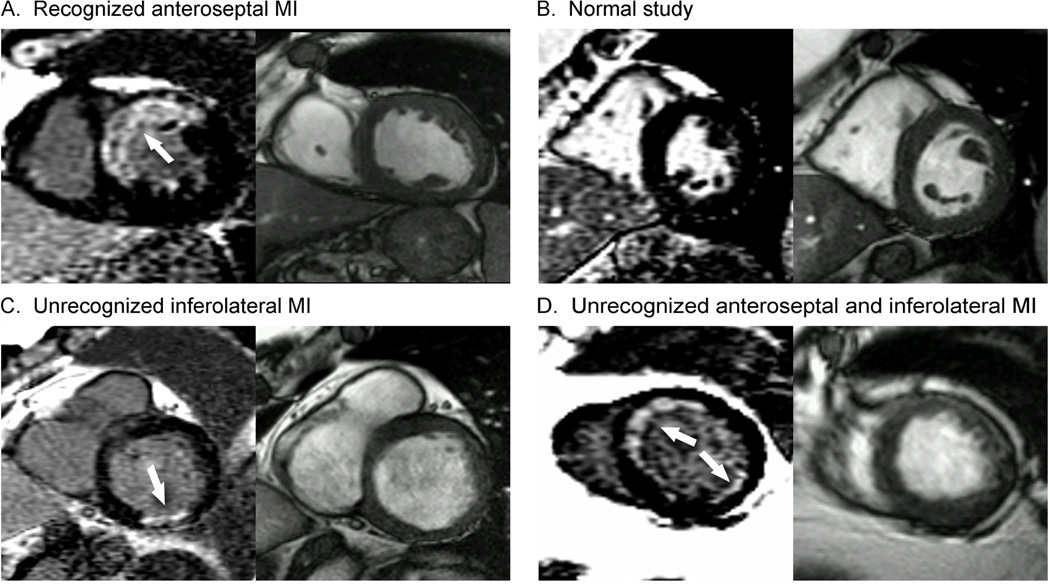
Context: Unrecognized myocardial infarction (MI) is prognostically important. Electrocardiography (ECG) has limited sensitivity for detecting unrecognized MI (UMI).
Objective: Determine prevalence and mortality risk for UMI detected by cardiac magnetic resonance (CMR) imaging or ECG among older individuals.
Design, setting, and participants: ICELAND MI is a cohort substudy of the Age, Gene/Environment Susceptibility-Reykjavik Study (enrollment January 2004-January 2007) using ECG or CMR to detect UMI. From a community-dwelling cohort of older individuals in Iceland, data for 936 participants aged 67 to 93 years were analyzed, including 670 who were randomly selected and 266 with diabetes.
Main outcome measures: Prevalence and mortality of MI through September 1, 2011. Results reported with 95% confidence limits and net reclassification improvement (NRI).
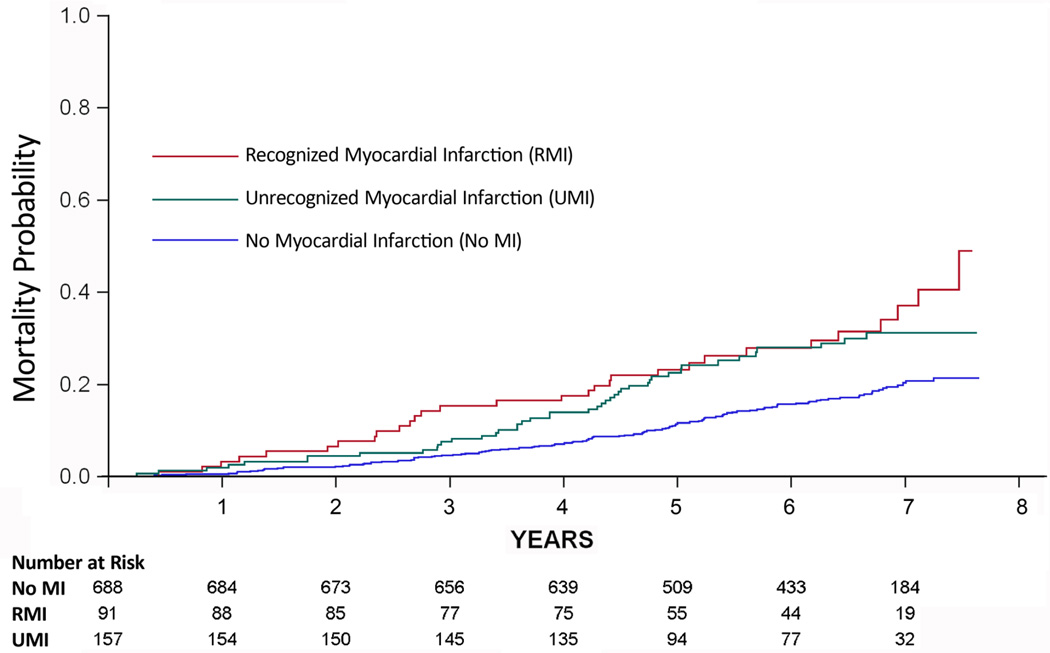
Results: Of 936 participants, 91 had recognized MI (RMI) (9.7%; 95% CI, 8% to 12%), and 157 had UMI detected by CMR (17%; 95% CI, 14% to 19%), which was more prevalent than the 46 UMI detected by ECG (5%; 95% CI, 4% to 6%; P < .001). Participants with diabetes (n = 337) had more UMI detected by CMR than by ECG (n = 72; 21%; 95% CI, 17% to 26%, vs n = 15; 4%; 95% CI, 2% to 7%; P < .001). Unrecognized MI by CMR was associated with atherosclerosis risk factors, coronary calcium, coronary revascularization, and peripheral vascular disease. Over a median of 6.4 years, 30 of 91 participants (33%; 95% CI, 23% to 43%) with RMI died, and 44 of 157 participants (28%; 95% CI, 21% to 35%) with UMI died, both higher rates than the 119 of 688 participants (17%; 95% CI, 15% to 20%) with no MI who died. Unrecognized MI by CMR improved risk stratification for mortality over RMI (NRI, 0.34; 95% CI, 0.16 to 0.53). Adjusting for age, sex, diabetes, and RMI, UMI by CMR remained associated with mortality (hazard ratio [HR], 1.45; 95% CI, 1.02 to 2.06, absolute risk increase [ARI], 8%) and significantly improved risk stratification for mortality (NRI, 0.16; 95% CI, 0.01 to 0.31), but UMI by ECG did not (HR, 0.88; 95% CI, 0.45 to 1.73; ARI, -2%; NRI, -0.05; 95% CI, -0.17 to 0.05). Compared with those with RMI, participants with UMI by CMR used cardiac medications such as statins less often (36%; 95% CI, 28% to 43%, or 56/157, vs 73%; 95% CI, 63% to 82%, or 66/91; P < .001).
Conclusions: In a community-based cohort of older individuals, the prevalence of UMI by CMR was higher than the prevalence of RMI and was associated with increased mortality risk. In contrast, UMI by ECG prevalence was lower than that of RMI and was not associated with increased mortality risk.
Trial registration: clinicaltrials.gov Identifier: NCT01322568.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Sigurdsson E, Thorgeirsson G, Sigvaldason H, Sigfusson N. Unrecognized myocardial infarction: epidemiology, clinical characteristics, and the prognostic role of angina pectoris. The Reykjavik Study. Annals of internal medicine. 1995 Jan 15;122(2):96–102. - PubMed
-
- Kannel WB, Abbott RD. Incidence and prognosis of unrecognized myocardial infarction. An update on the Framingham study. N Engl J Med. 1984 Nov 1;311(18):1144–1147. - PubMed
-
- Sheifer SE, Gersh BJ, Yanez ND, 3rd, Ades PA, Burke GL, Manolio TA. Prevalence, predisposing factors, and prognosis of clinically unrecognized myocardial infarction in the elderly. J Am Coll Cardiol. 2000 Jan;35(1):119–126. - PubMed
-
- Boland LL, Folsom AR, Sorlie PD, et al. Occurrence of unrecognized myocardial infarction in subjects aged 45 to 65 years (the ARIC study) Am J Cardiol. 2002 Nov 1;90(9):927–931. - PubMed
-
- Kim RJ, Wu E, Rafael A, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000 Nov 16;343(20):1445–1453. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
