

Improved long-term survival after major resection for hepatocellular carcinoma: a multicenter analysis based on a new definition of major hepatectomy
- PMID: 22948836
- PMCID: PMC3880185
- DOI: 10.1007/s11605-012-2005-4
Improved long-term survival after major resection for hepatocellular carcinoma: a multicenter analysis based on a new definition of major hepatectomy
Abstract
Background: Advances in the surgical management of hepatocellular carcinoma (HCC) have expanded the indications for curative hepatectomy, including more extensive liver resections. The purpose of this study was to examine long-term survival trends for patients treated with major hepatectomy for HCC.
Patients and methods: Clinicopathologic data for 1,115 patients with HCC who underwent hepatectomy between 1981 and 2008 at five hepatobiliary centers in France, China, and the USA were assessed. In addition to other performance metrics, outcomes were evaluated using resection of ≥4 liver segments as a novel definition of major hepatectomy.
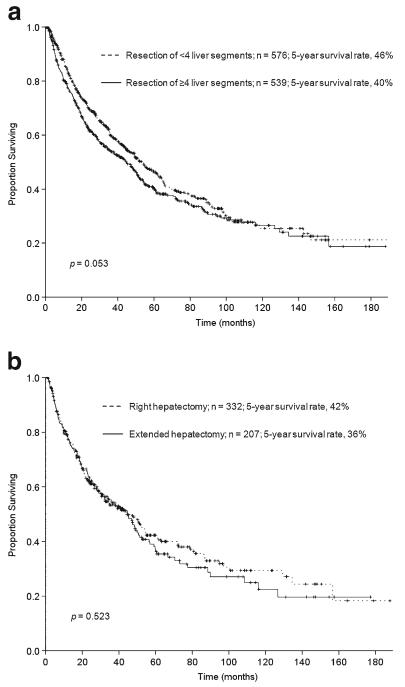
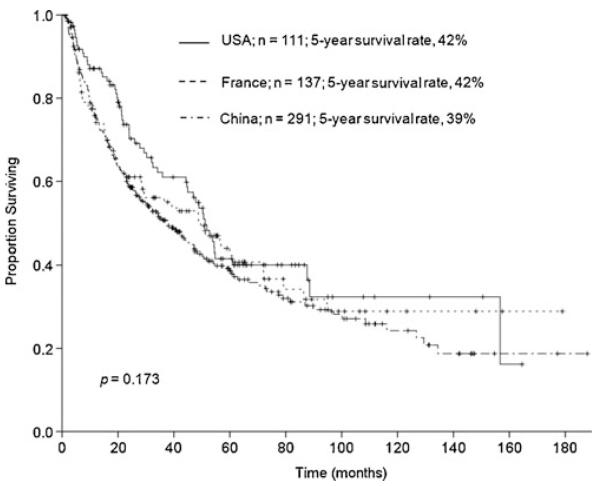
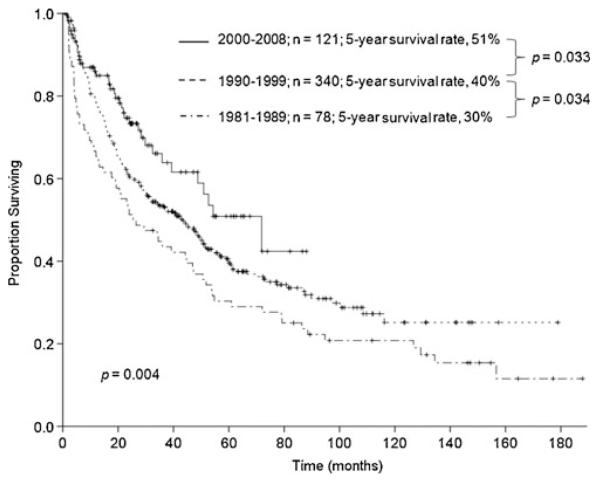
Results: Major hepatectomy was performed in 539 patients. In the major hepatectomy group, median tumor size was 10 cm (range: 1-27 cm) and 22 % of the patients had bilateral lesions. The TNM Stage distribution included 29 % Stage I, 31 % Stage II, 38 % Stage III, and 2 % Stage IV. The postoperative histologic examination indicated that chronic liver disease was present in 35 % of the patients and tumor microvascular invasion was identified in 60 % of the patients. The 90-day postoperative mortality rate was 4 %. After a median follow-up time of 63 months, the 5-year overall survival rate was 40 %. Patients treated with right hepatectomy (n = 332) and those requiring extended hepatectomy (n = 207) had similar 90-day postoperative mortality rates (4 % and 4 %, respectively, p = 0.976) and 5-year overall survival rates (42 % and 36 %, respectively, p = 0.523). Postoperative mortality and overall survival rates after major hepatectomy were similar among the participating countries (p > 0.1) and improved over time with 5-year survival rates of 30 %, 40 %, and 51 % for the years 1981-1989, 1990-1999, and the most recent era of 2000-2008, respectively (p = 0.004). In multivariate analysis, factors that were significantly associated with worse survivals included AFP level >1,000 ng/mL, tumor size >5 cm, presence of major vascular invasion, presence of extrahepatic metastases, positive surgical margins, and earlier time period in which the major hepatectomy was performed.
Conclusions: This multinational, long-term HCC survival analysis indicates that expansion of surgical indications to include major hepatectomy is justified by the significant improvement in outcomes over the past three decades observed in both the East and the West.
Figures
References
-
- Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. - PubMed
-
- Livraghi T, Meloni F, Di Stasi M, et al. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: Is resection still the treatment of choice? Hepatology. 2008;47:82–89. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
