

Adherence to antiretroviral therapy during and after pregnancy in low-income, middle-income, and high-income countries: a systematic review and meta-analysis
- PMID: 22951634
- PMCID: PMC5061936
- DOI: 10.1097/QAD.0b013e328359590f
Adherence to antiretroviral therapy during and after pregnancy in low-income, middle-income, and high-income countries: a systematic review and meta-analysis
Abstract
Objective: To estimate antiretroviral therapy (ART) adherence rates during pregnancy and postpartum in high-income, middle-income, and low-income countries.
Design: Systematic review and meta-analysis.
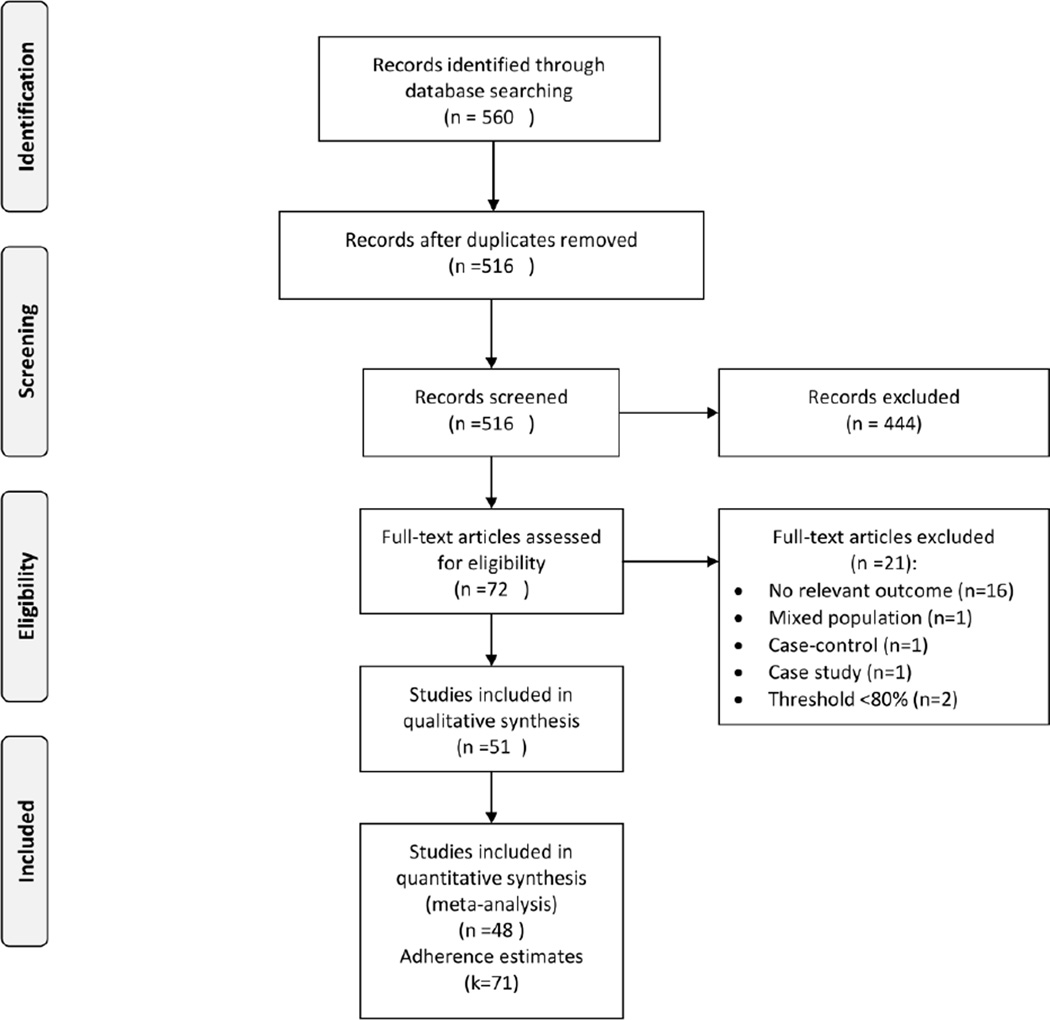
Methods: MEDLINE, EMBASE, SCI Web of Science, NLM Gateway, and Google scholar databases were searched. We included all studies reporting adherence rates as a primary or secondary outcome among HIV-infected pregnant women. Two independent reviewers extracted data on adherence and study characteristics. A random-effects model was used to pool adherence rates; sensitivity, heterogeneity, and publication bias were assessed.
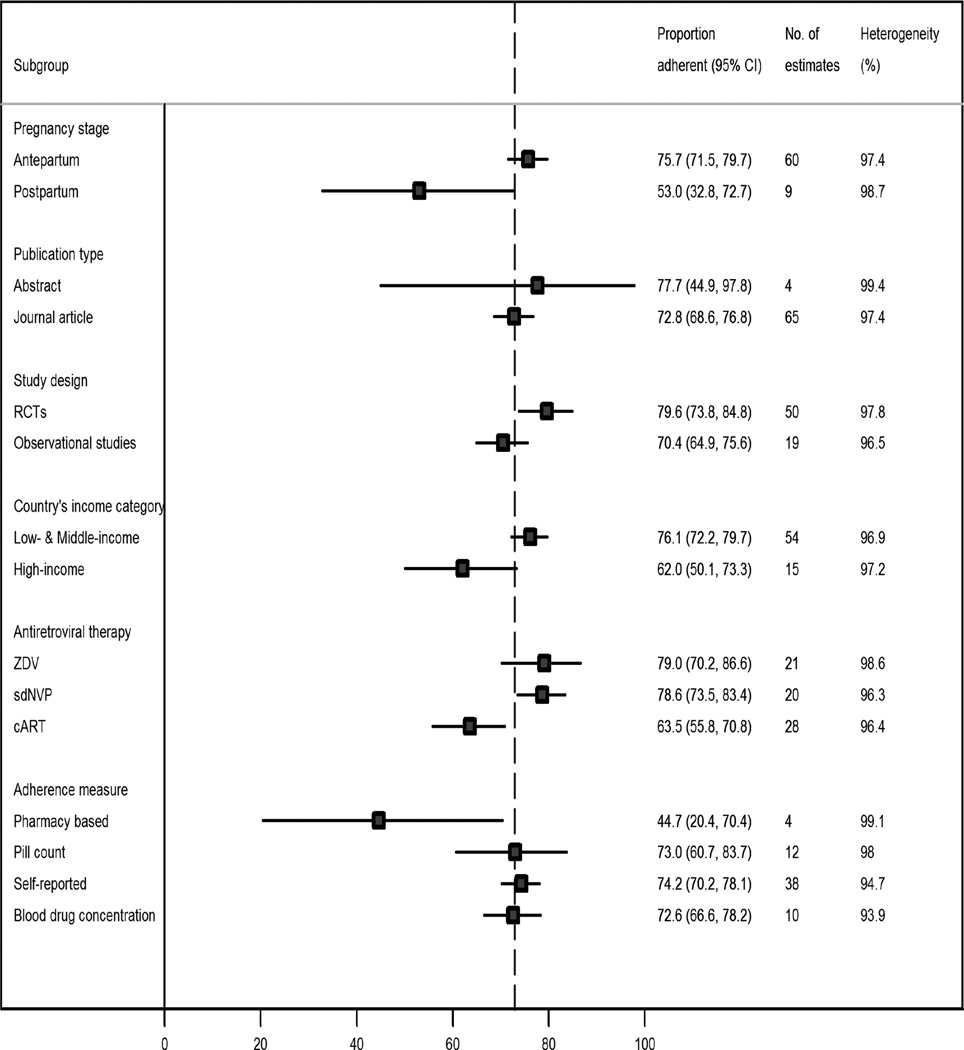
Results: Of 72 eligible articles, 51 studies involving 20 153 HIV-infected pregnant women were included. Most studies were from United States (n = 14, 27%) followed by Kenya (n = 6, 12%), South Africa (n = 5, 10%), and Zambia (n = 5, 10%). The threshold defining good adherence to ART varied across studies (>80, >90, >95, 100%). A pooled analysis of all studies indicated a pooled estimate of 73.5% [95% confidence interval (CI) 69.3-77.5%] of pregnant women who had adequate (>80%) ART adherence. The pooled proportion of women with adequate adherence levels was higher during the antepartum (75.7%, 95% CI 71.5-79.7%) than during postpartum (53.0%, 95% CI 32.8-72.7%; P = 0.005). Selected reported barriers for nonadherence included physical, economic and emotional stresses, depression (especially postdelivery), alcohol or drug use, and ART dosing frequency or pill burden.
Conclusion: Our findings indicate that only 73.5% of pregnant women achieved optimal ART adherence. Reaching adequate ART adherence levels was a challenge in pregnancy, but especially during the postpartum period. Further research to investigate specific barriers and interventions to address them is urgently needed globally.
Conflict of interest statement
Conflict of Interest/Disclosures: None
Figures


References
-
- World Health Organization. Towards Universal Access: Scaling up priority HIV/AIDS interventions in the health sector, progress report 2010. Geneva, Switzerland: World Health Organization; 2010.
-
- Townsend CL, Cortina-Borja M, Peckham CS, de Ruiter A, Lyall H, Tookey PA. Low rates of mother-to-child transmission of HIV following effective pregnancy interventions in the United Kingdom and Ireland, 2000–2006. AIDS. 2008;22:973–981. - PubMed
-
- De Cock KM, Fowler MG, Mercier E, de Vincenzi I, Saba J, Hoff E, et al. Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy and practice. JAMA. 2000;283:1175–1182. - PubMed
-
- Wiktor SZ, Ekpini E, Nduati RW. Prevention of mother-to-child transmission of HIV-1 in Africa. AIDS. 1997;11(Suppl B):S79–S87. - PubMed
-
- World Health Organization. Antiretroviral drugs for treating pregnant women and preventing HIV infections in infants: recommendations for a public health approach: 2010 version. Geneva, Switzerland: World Health Organization; 2010. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
