

Clinical and neuroanatomical predictors of cerebellar mutism syndrome
- PMID: 22952198
- PMCID: PMC3452341
- DOI: 10.1093/neuonc/nos160
Clinical and neuroanatomical predictors of cerebellar mutism syndrome
Abstract
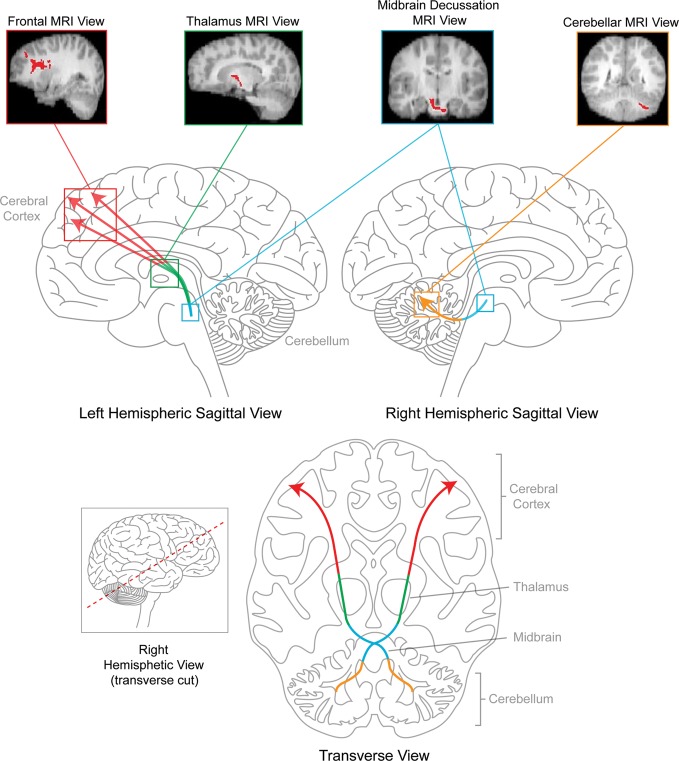
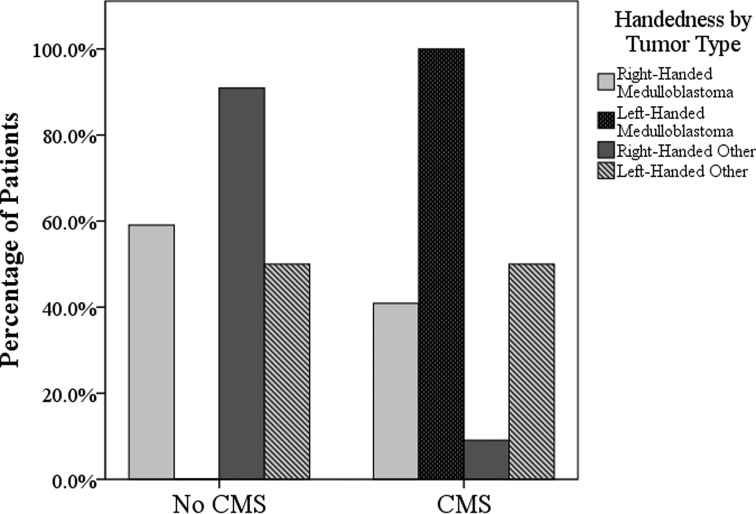
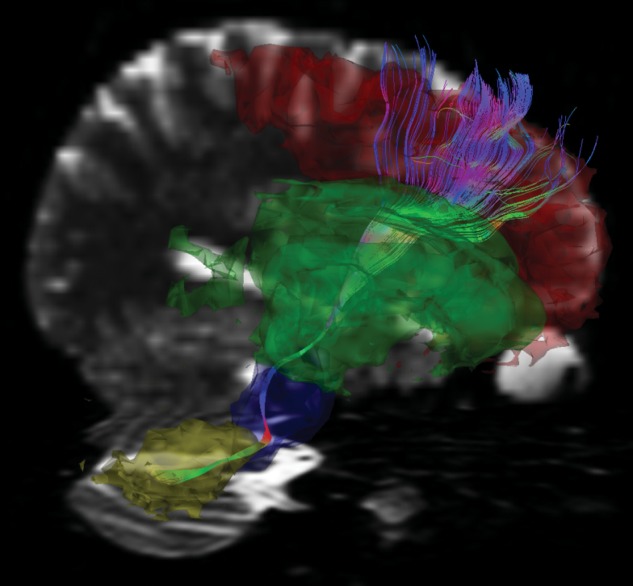
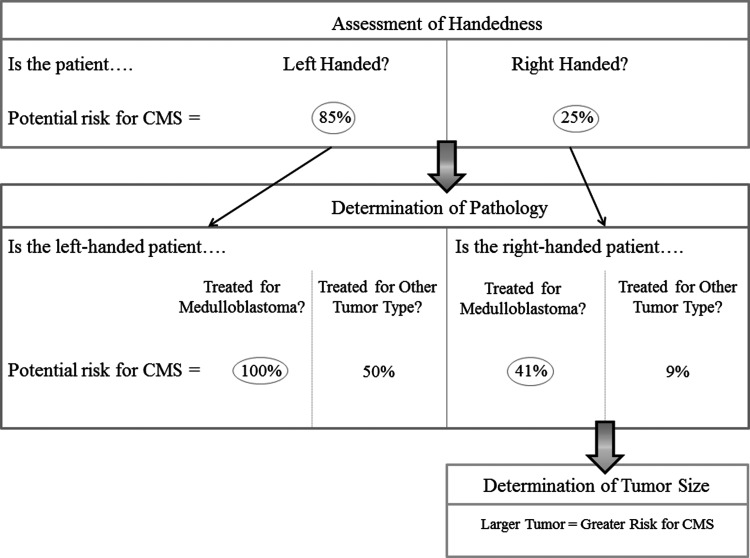
Cerebellar mutism syndrome (CMS) is an important medical challenge in the management of pediatric posterior fossa brain tumors, because it occurs in a subset of children following tumor resection. A definitive clinical profile and neuroanatomical substrate associated with CMS remains unclear. We investigated the relationship between presurgical and clinical variables and the incidence of CMS, along with diffusion tensor imaging, to characterize the integrity of cerebello-thalamo-cerebral white matter pathways. Seventeen children with posterior fossa tumors and CMS, 34 children with posterior fossa tumors without CMS, and 28 healthy children were enrolled in this study. Bilateral cerebello-thalamo-cerebral pathways were delineated and segmented into anatomical regions. Mean integrity measures for each region were compared among children with CMS, children without CMS, and healthy children. Left-handedness, medulloblastoma histology, and larger tumor size distinguished between patients with CMS and patients without CMS (P < .04). Right cerebellar white matter within the cerebello-thalamo-cerebral pathway was compromised in children with CMS relative to children without CMS and healthy children (P < .02). We provide a potential schema for CMS risk among children treated for posterior fossa tumors. Left-handed children treated for medulloblastoma may be the most at risk for CMS, and unilateral, localized damage within the cerebello-thalamo-cerebral pathway at the level of the right cerebellum is implicated in the presentation of CMS. This disruption in communication between the right cerebellum and left frontal cortex may contribute to speech-language problems observed in children with CMS. Our findings may be relevant for surgical planning and speech-language therapy to mitigate symptoms of CMS.
Figures
References
-
- Van Calenbergh F, Van de Laar A, Plets C, Goffin J, Casaer P. Transient cerebellar mutism after posterior fossa surgery in children. Neurosurgery. 1995;37(5):894–898. - PubMed
-
- Pollack IF. Posterior fossa syndrome. Int Rev Neurobiol. 1997;41:411–432. - PubMed
-
- Robertson PL, Muraszko KM, Holmes EJ, et al. Incidence and severity of postoperative cerebellar mutism syndrome in children with medulloblastoma: a prospective study by the Children's Oncology Group. J Neurosurg. 2006;105(Suppl 6):444–451. - PubMed
-
- Riva D, Giorgi C. The cerebellum contributes to higher functions during development: evidence from a series of children surgically treated for posterior fossa tumours. Brain. 2000;123(5):1051–1061. - PubMed
-
- Vandeinse D, Hornyak JE. Linguistic and cognitive deficits associated with cerebellar mutism. Pediatr Rehabil. 1997;1(1):41–44. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
