

Lumbosacral transitional vertebrae: association with low back pain
- PMID: 22952380
- PMCID: PMC3480814
- DOI: 10.1148/radiol.12112747
Lumbosacral transitional vertebrae: association with low back pain
Abstract
Purpose: To assess the prevalence and degree of lumbosacral transitional vertebrae (LSTV) in the Osteoarthritis Initiative (OAI) cohort, to assess whether LSTV correlates with low back pain (LBP) and buttock pain, and to assess the reproducibility of grading LSTV.
Materials & methods: Institutional review board approval was obtained, and informed consent documentation was approved for the study protocol. Standard standing pelvic radiographs that included the transverse processes of L5 were graded according to Castellvi classification of LSTV in 4636 participants (1992 men and 2804 women; aged 45-80 years) from the OAI cohort. These data were correlated with prevalence and severity of LBP and buttock pain.
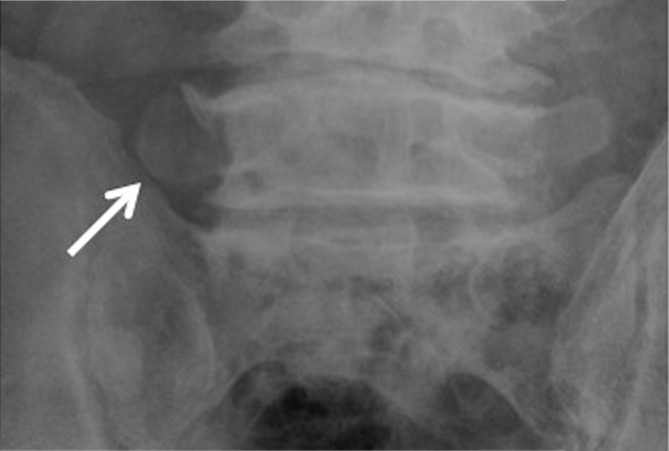
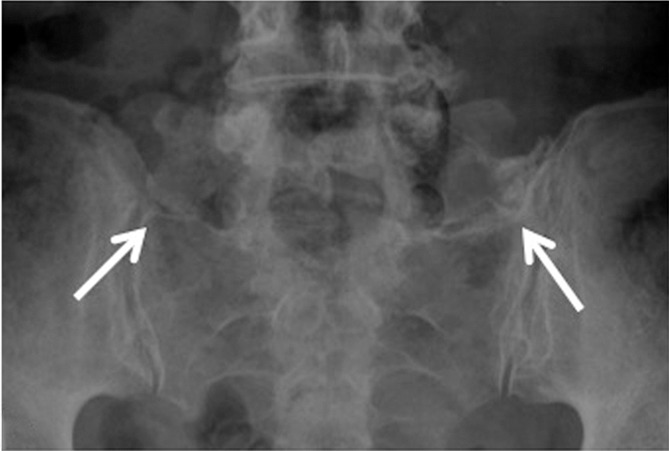
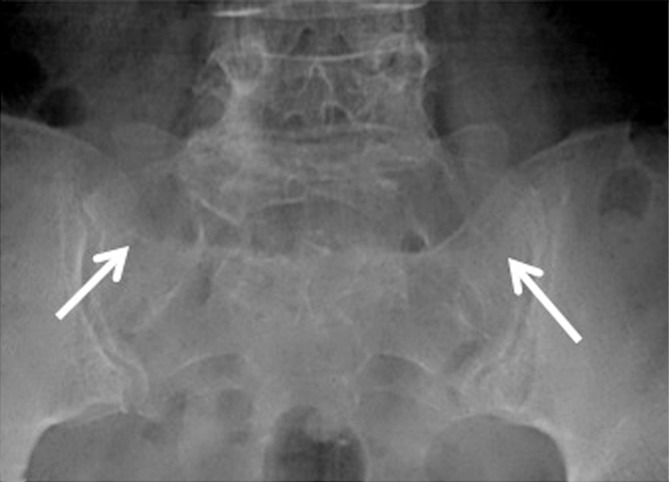
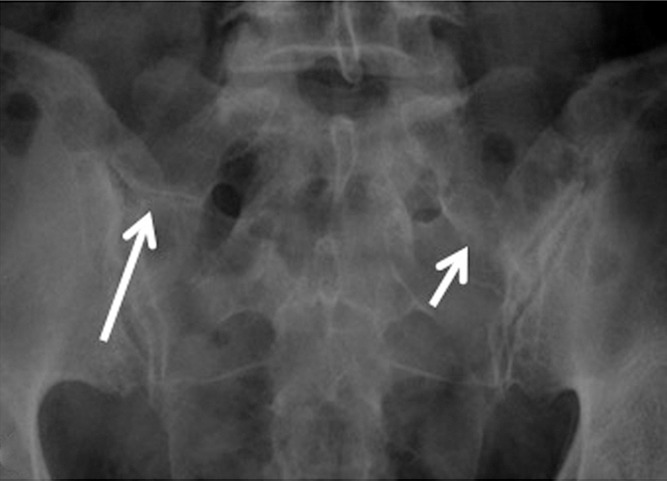
Results: Prevalence of LSTV was 18.1% (841 of 4636), with a higher rate in men than in women (28.1% vs 11.1%, respectively; P<.001). Of the 841 individuals with LSTV, 41.72% were type I (dysplastic enlarged transverse process), 41.4% were type II (pseudoarticulation), 11.5% were type III (fusion), and 5.2% were type IV (one transverse process fused and one with pseudoarticulation). Of the participants without LSTV, 53.9% reported LBP, while the prevalence of LBP for types I, II, III, and IV was 46%, 73%, 40%, and 66%, respectively (P<.05, χ2 test). Types II and IV had higher prevalence and severity of LBP and buttock pain (P<.001).
Conclusion: LSTV types II and IV positively correlate with prevalence and severity of LBP and buttock pain.
© RSNA, 2012
Figures
References
-
- Becker A, Held H, Redaelli M, et al. Low back pain in primary care: costs of care and prediction of future health care utilization. Spine 2010;35(18):1714–1720 - PubMed
-
- Luo X, Pietrobon R, Sun SX, Liu GG, Hey L. Estimates and patterns of direct health care expenditures among individuals with back pain in the United States. Spine 2004;29(1):79–86 - PubMed
-
- Frymoyer JW, Cats-Baril WL. An overview of the incidences and costs of low back pain. Orthop Clin North Am 1991;22(2):263–271 - PubMed
-
- Stewart WF, Ricci JA, Chee E, Morganstein D, Lipton R. Lost productive time and cost due to common pain conditions in the US workforce. JAMA 2003;290(18):2443–2454 - PubMed
-
- Deyo RA, Weinstein JN. Low back pain. N Engl J Med 2001;344(5):363–370 - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
