

Child mortality estimation: a comparison of UN IGME and IHME estimates of levels and trends in under-five mortality rates and deaths
- PMID: 22952434
- PMCID: PMC3429386
- DOI: 10.1371/journal.pmed.1001288
Child mortality estimation: a comparison of UN IGME and IHME estimates of levels and trends in under-five mortality rates and deaths
Abstract
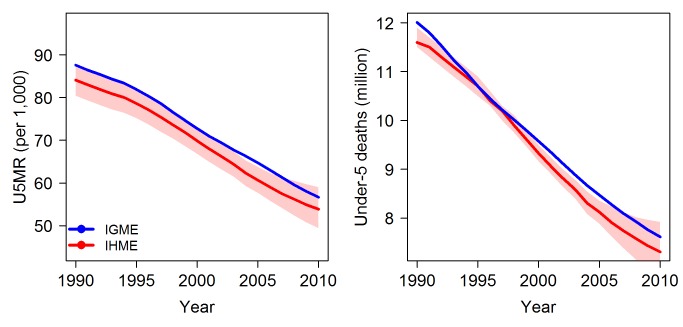
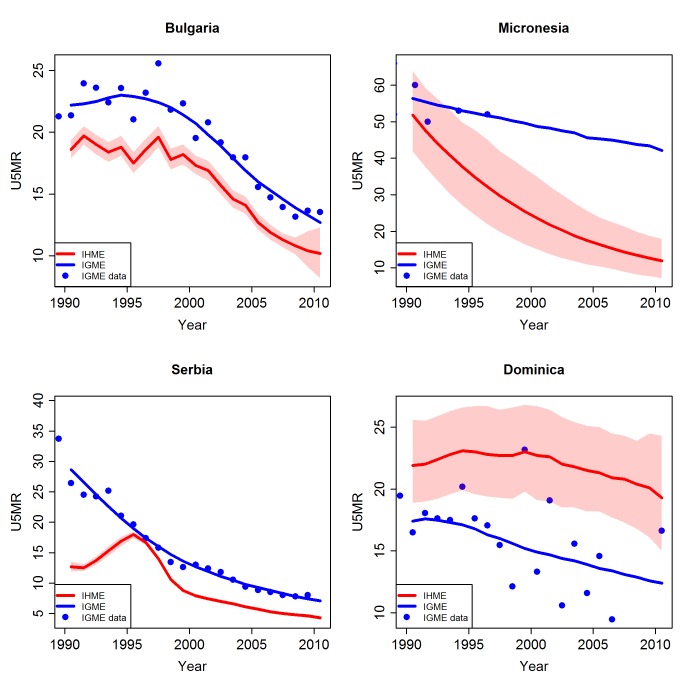
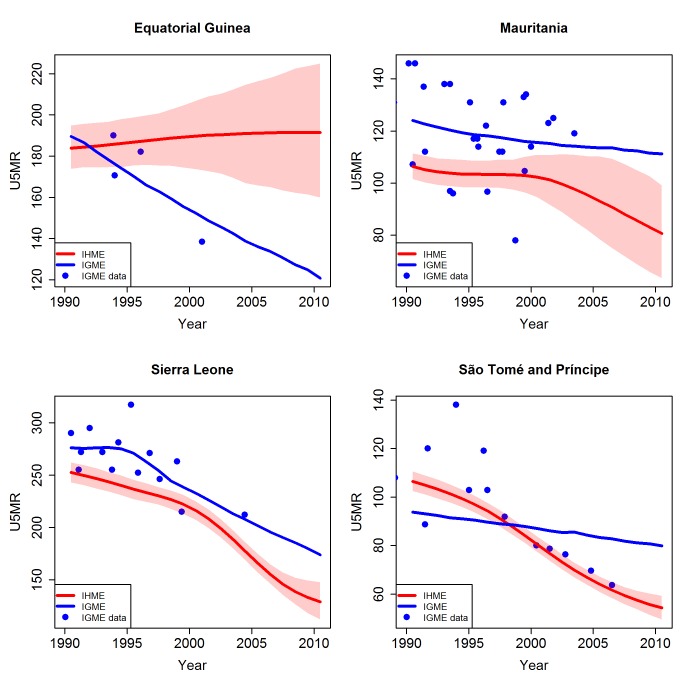
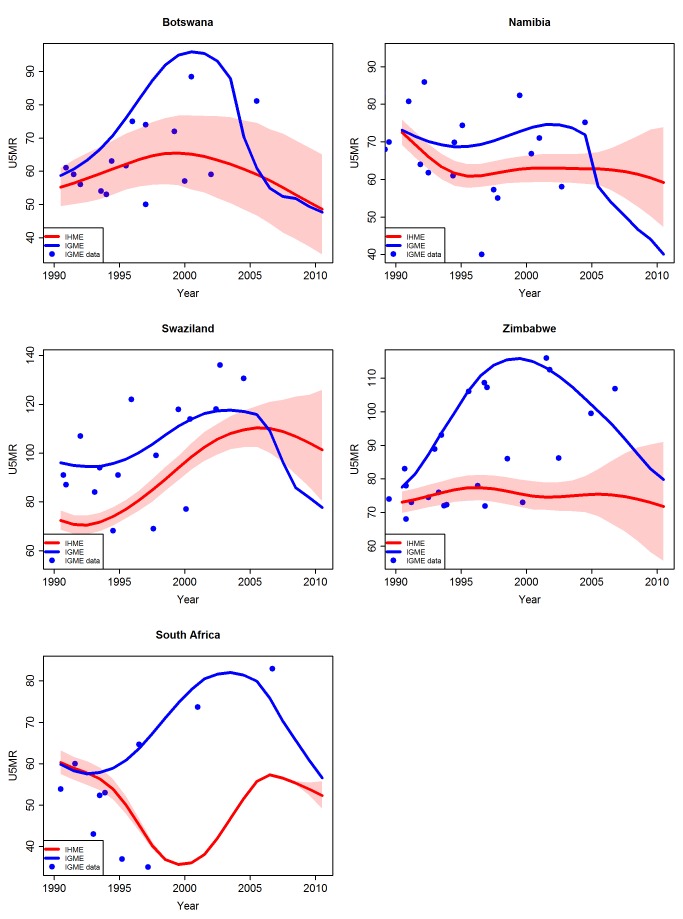
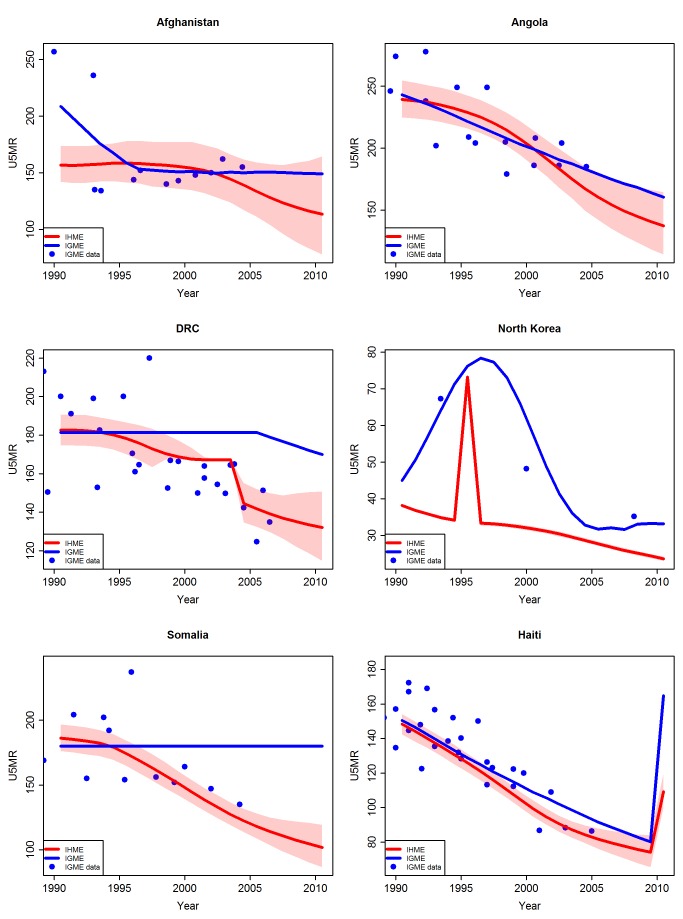
Background: Millennium Development Goal 4 calls for a reduction in the under-five mortality rate (U5MR) by two-thirds between 1990 and 2015. In 2011, estimates were published by the United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) and the Institute for Health Metrics and Evaluation (IHME). The difference in the U5MR estimates produced by the two research groups was more than 10% and corresponded to more than ten deaths per 1,000 live births for 10% of all countries in 1990 and 20% of all countries in 2010, which can lead to conflicting conclusions with respect to countries' progress. To understand what caused the differences in estimates, we summarised differences in underlying data and modelling approaches used by the two groups, and analysed their effects.
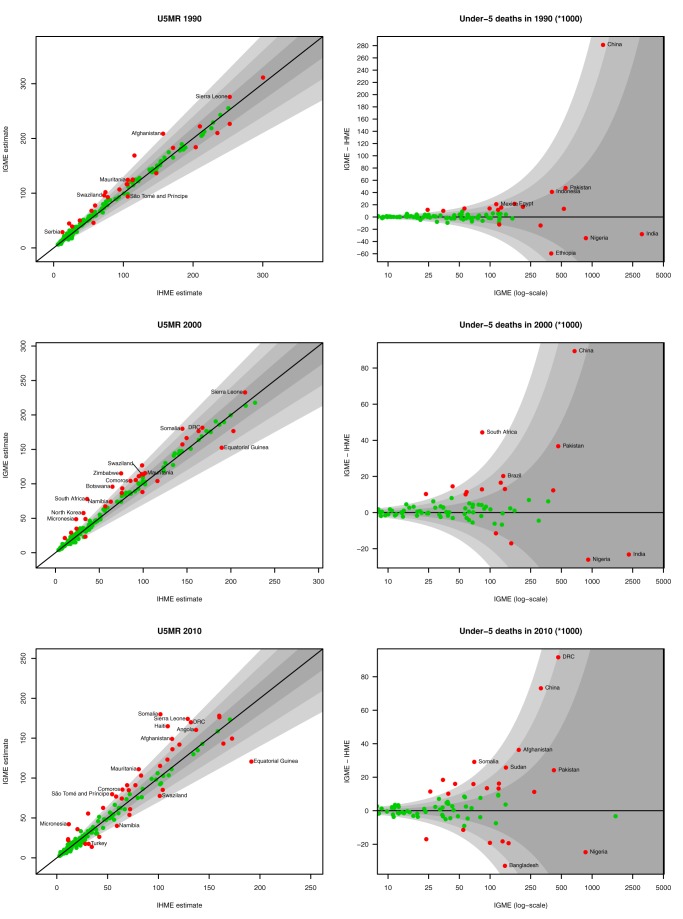
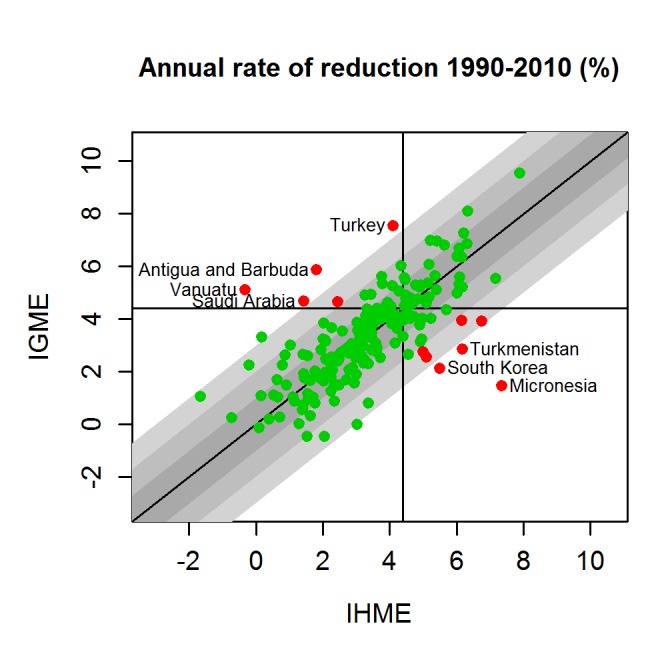
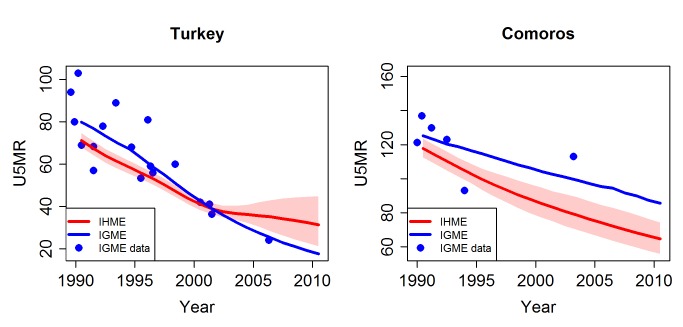
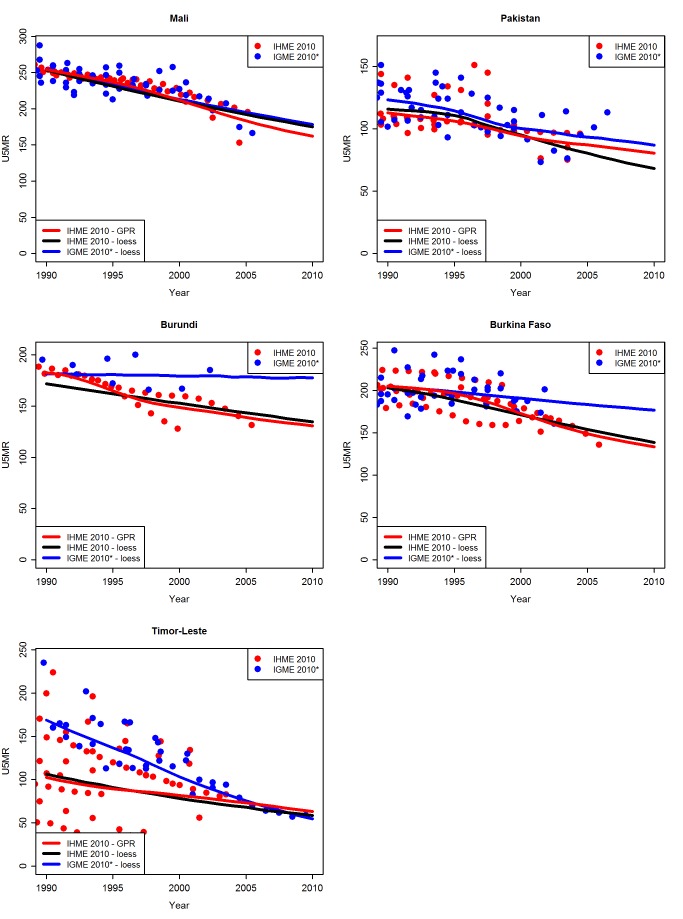
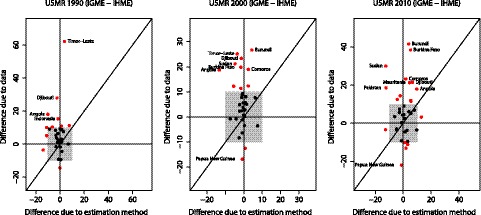
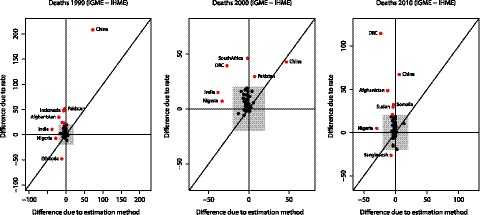
Methods and findings: UN IGME and IHME estimation approaches differ with respect to the construction of databases and the pre-processing of data, trend fitting procedures, inclusion and exclusion of data series, and additional adjustment procedures. Large differences in U5MR estimates between the UN IGME and the IHME exist in countries with conflicts or civil unrest, countries with high HIV prevalence, and countries where the underlying data used to derive the estimates were different, especially if the exclusion of data series differed between the two research groups. A decomposition of the differences showed that differences in estimates due to using different data (inclusion of data series and pre-processing of data) are on average larger than the differences due to using different trend fitting methods.
Conclusions: Substantial country-specific differences between UN IGME and IHME estimates for U5MR and the number of under-five deaths exist because of various differences in data and modelling assumptions used. Often differences are illustrative of the lack of reliable data and likely to decrease as more data become available. Improved transparency on methods and data used will help to improve understanding about the drivers of the differences. Please see later in the article for the Editors' Summary.
Conflict of interest statement
LA is a member of the technical advisory group of the UN IGME. DY is working at the United Nations Children's Fund which is a lead member of the UN IGME. The views expressed in this paper are those of the authors and do not necessarily reflect the views of the United Nations Children's Fund.
Figures
References
-
- United Nations Children's Fund (2011) Levels & trends in child mortality: report 2011. Estimates developed by the UN Inter-agency Group for Child Morality Estimation. New York: United Nations Children's Fund.
-
- Lozano R, Wang H, Foreman KJ, Rajaratnam JK, Naghavi M, et al. (2011) Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. Lancet 378: 1139–1165. - PubMed
-
- Boerma JT, Mathers C, Abou-Zahr C (2010) WHO and global health monitoring: the way forward. PLoS Med 7: e1000373 doi:10.1371/journal.pmed.1000373. - DOI - PMC - PubMed
-
- Murray CJL, Lopez AD (2010) Production and analysis of health indicators: the role of academia. PLoS Med 7: e1001004 doi:10.1371/journal.pmed.1001004. - DOI - PMC - PubMed
-
- Department of International Economic and Social Affairs (1983) Manual X—indirect techniques for demographic estimation. New York: United Nations.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
