

The spectrum of central nervous system infections in an adult referral hospital in Hanoi, Vietnam
- PMID: 22952590
- PMCID: PMC3431395
- DOI: 10.1371/journal.pone.0042099
The spectrum of central nervous system infections in an adult referral hospital in Hanoi, Vietnam
Abstract
Objectives: To determine prospectively the causative pathogens of central nervous system (CNS) infections in patients admitted to a tertiary referral hospital in Hanoi, Vietnam.
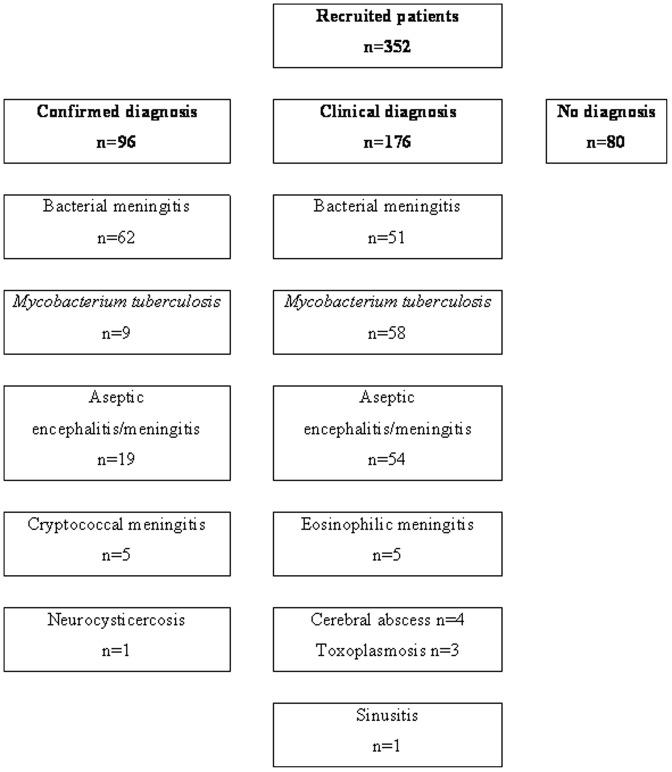
Methods: From May 2007 to December 2008, cerebrospinal fluid (CSF) samples from 352 adults with suspected meningitis or encephalitis underwent routine testing, staining (Gram, Ziehl-Nielsen, India ink), bacterial culture and polymerase chain reaction targeting Neisseria meningitidis, Streptococcus pneumoniae, S. suis, Haemophilus influenzae type b, Herpes simplex virus (HSV), Varicella Zoster virus (VZV), enterovirus, and 16S ribosomal RNA. Blood cultures and clinically indicated radiology were also performed. Patients were classified as having confirmed or suspected bacterial (BM), tuberculous (TBM), cryptococcal (CRM), eosinophilic (EOM) meningitis, aseptic encephalitis/meningitis (AEM), neurocysticercosis and others.
Results: 352 (male: 66%) patients were recruited: median age 34 years (range 13-85). 95/352 (27.3%) diagnoses were laboratory confirmed and one by cranial radiology: BM (n = 62), TBM (n = 9), AEM (n = 19), CRM (n = 5), and neurocysticercosis (n = 1, cranial radiology). S. suis predominated as the cause of BM [48/62 (77.4%)]; Listeria monocytogenese (n = 1), S. pasteurianus (n = 1) and N. meningitidis (n = 2) were infrequent. AEM viruses were: HSV (n = 12), VZV (n = 5) and enterovirus (n = 2). 5 patients had EOM. Of 262/352 (74.4%) patients with full clinical data, 209 (79.8%) were hospital referrals and 186 (71%) had been on antimicrobials. 21 (8%) patients died: TBM (15.2%), AEM (10%), and BM (2.8%).
Conclusions: Most infections lacked microbiological confirmation. S. suis was the most common cause of BM in this setting. Improved diagnostics are needed for meningoencephalitic syndromes to inform treatment and prevention strategies.
Conflict of interest statement
Figures
References
-
- Hosoglu S, Geyik MF, Balik I, Aygen B, Erol S, et al. (2003) Tuberculous meningitis in adults in Turkey: epidemiology, diagnosis, clinic and laboratory [corrected]. Eur J Epidemiol 18: 337–343. - PubMed
-
- Ooi MH, Lewthwaite P, Lai BF, Mohan A, Clear D, et al. (2008) The epidemiology, clinical features, and long-term prognosis of Japanese encephalitis in central sarawak, malaysia, 1997–2005. Clin Infect Dis 47: 458–468. - PubMed
-
- Punyagupta S, Bunnag T, Juttijudata P (1990) Eosinophilic meningitis in Thailand. Clinical and epidemiological characteristics of 162 patients with myeloencephalitis probably caused by Gnathostoma spinigerum. J Neurol Sci 96: 241–256. - PubMed
-
- Mai NT, Hoa NT, Nga TV, Linh le D, Chau TT, et al. (2008) Streptococcus suis meningitis in adults in Vietnam. Clin Infect Dis 46: 659–667. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
