

Enzyme-linked immunosorbent assay to diagnose human leptospirosis: a meta-analysis of the published literature
- PMID: 22953720
- PMCID: PMC9152066
- DOI: 10.1017/S0950268812001951
Enzyme-linked immunosorbent assay to diagnose human leptospirosis: a meta-analysis of the published literature
Abstract
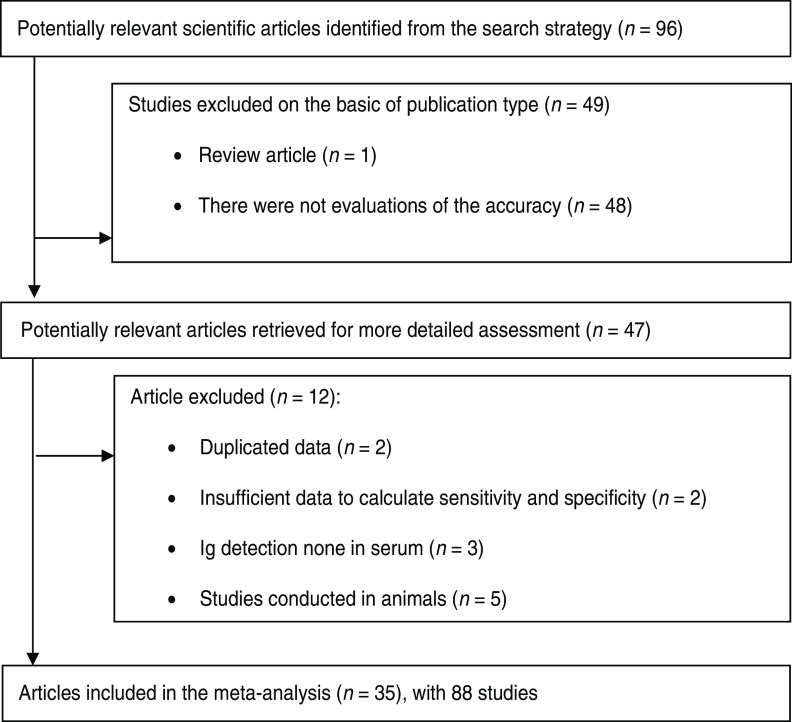
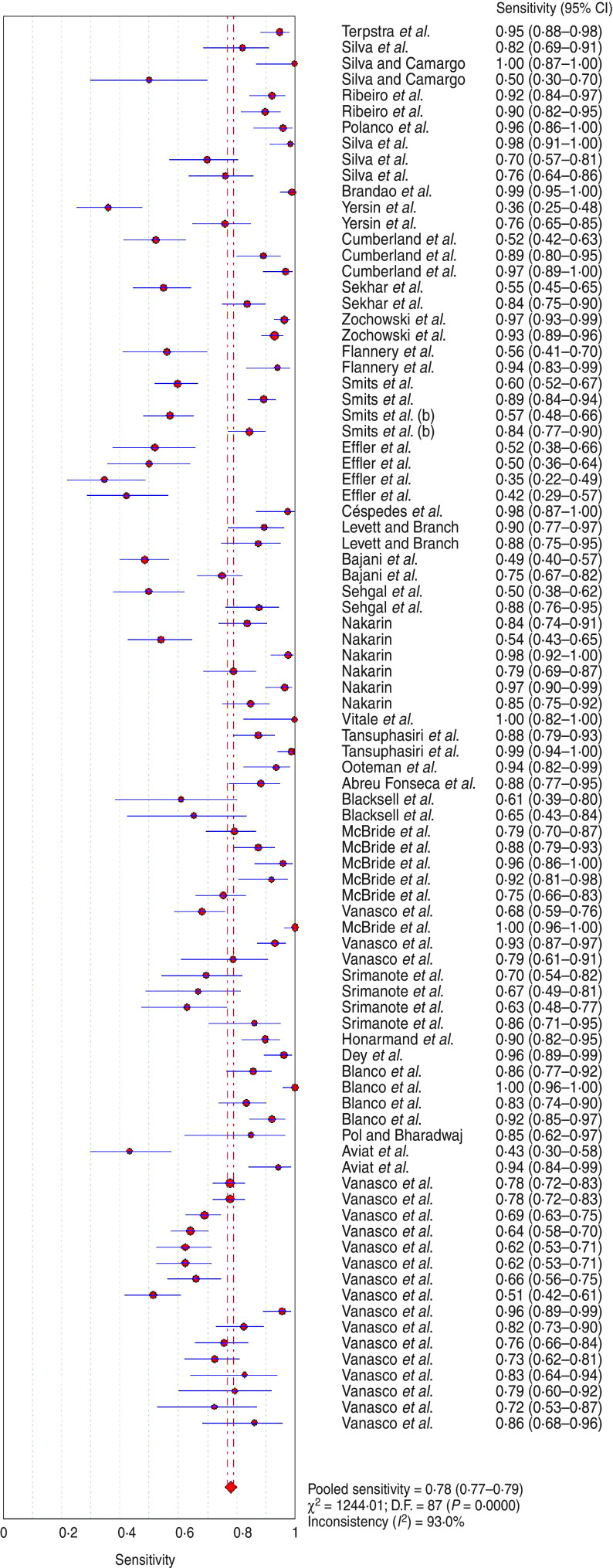
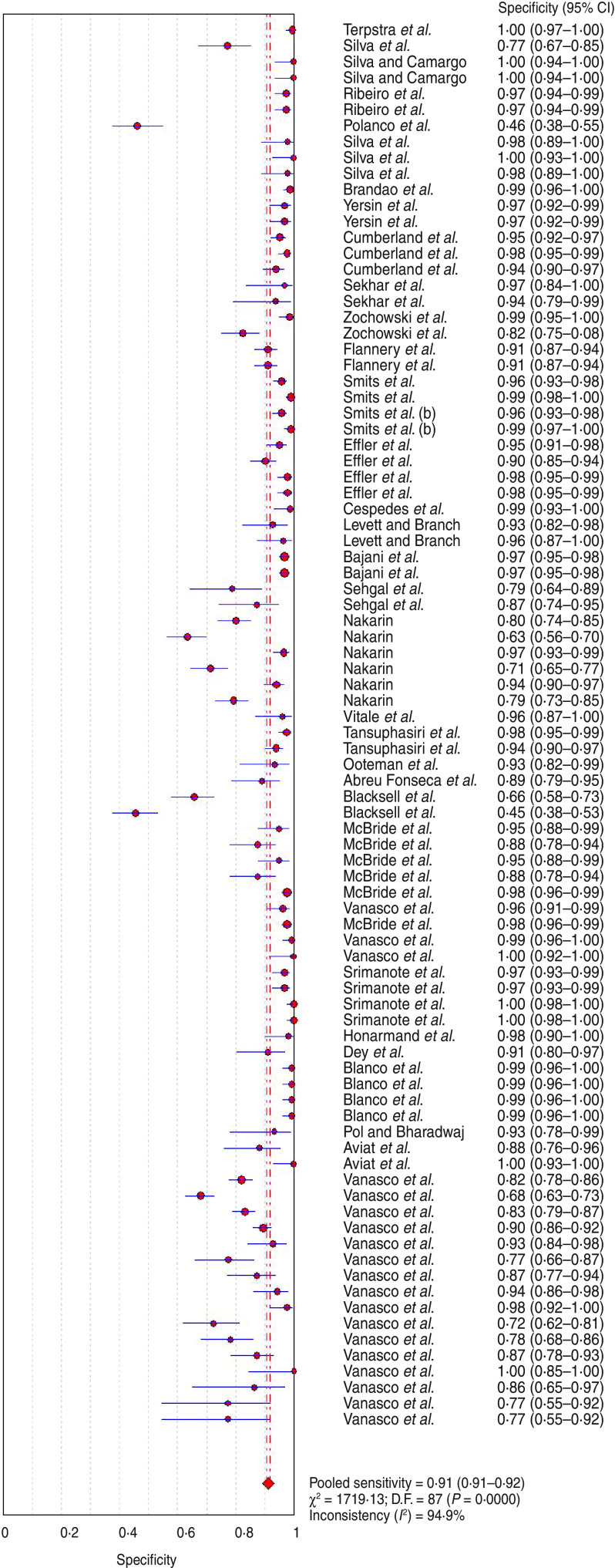
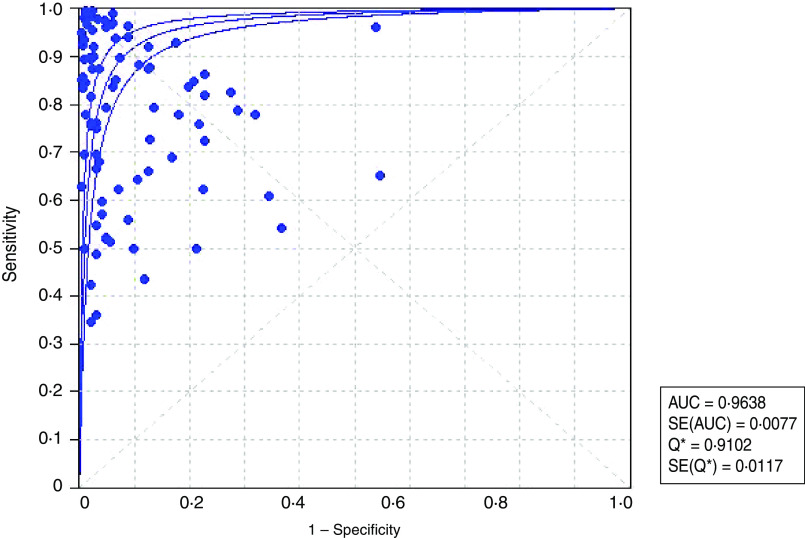
We report an evaluation of the accuracy of ELISA for the detection of Leptospira-specific antibodies in humans. Eighty-eight studies published in 35 articles met all inclusion criteria and were submitted to meta-analysis. Pooled sensitivity and specificity were 0·779 (95% CI 0·770-0·789) and 0·913 (95% CI 0·908-0·917), respectively, and the area under the curve was 0·964. Heterogeneity across studies was statistically significant, but none of the sources of heterogeneity (disease stage, antigen used, antibody detected) could fully explain this finding. Although the convalescent stage of disease was significantly associated with higher diagnostic accuracy, IgM ELISA was the best choice, regardless of the stage of disease. Negative ELISAs (IgG or IgM) applied in the acute phase do not rule out leptospirosis due to the possibility of false-negative results. In this case it is advisable to request a second blood sample or to apply a direct method for leptospiral DNA.
Figures
References
-
- McBride AJA, et al. Leptospirosis. Current Opinion on Infectious Diseases 2005; 18: 376–386. - PubMed
-
- Sehgal SC, et al. Field application of Lepto lateral flow for rapid diagnosis of leptospirosis. Journal of Medicine and Microbiology 2003; 52: 897–901. - PubMed
-
- Aviat F, et al. Synthetic peptide issued from Hap1/LipL32 for new early serodiagnosis of human leptospirosis. Comparative Immunology, Microbiology and Infectious Diseases 2010; 33: 375–387. - PubMed
-
- Vanasco NB, et al. Clinical characteristics and risk factors of human leptospirosis in Argentina (1999–2005). Acta Tropica 2008; 107: 255–258. - PubMed
-
- Smits HL, et al. Latex based, rapid and easy assay for human leptospirosis in a single test format. Tropical Medicine and International Health 2001; 6: 114–118. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
