

Ginkgo biloba does not improve cognitive function in MS: a randomized placebo-controlled trial
- PMID: 22955125
- PMCID: PMC3440446
- DOI: 10.1212/WNL.0b013e31826aac60
Ginkgo biloba does not improve cognitive function in MS: a randomized placebo-controlled trial
Abstract
Objective: To determine whether Ginkgo biloba extract (ginkgo) improves cognitive function in persons with multiple sclerosis (MS).
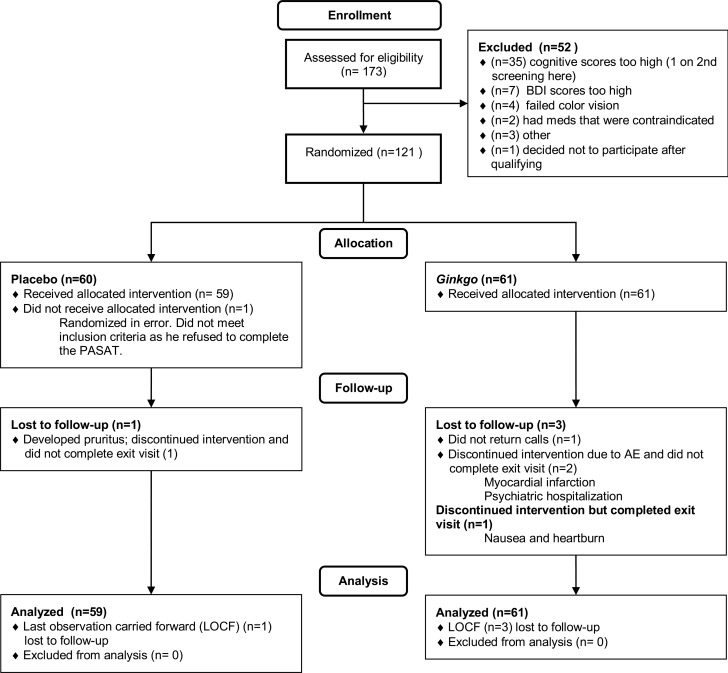
Methods: Persons with MS from the Seattle and Portland VA clinics and adjacent communities who scored 1 SD or more below the mean on one of 4 neuropsychological tests (Stroop Test, California Verbal Learning Test II [CVLT-II], Controlled Oral Word Association Test [COWAT], and Paced Auditory Serial Addition Task [PASAT]) were randomly assigned to receive either one 120-mg tablet of ginkgo (EGb-761; Willmar Schwabe GmbH & Co, Germany) or one placebo tablet twice a day for 12 weeks. As the primary outcome, we compared the performance of the 2 groups on the 4 tests at exit after adjusting for baseline performance.
Results: Fifty-nine subjects received placebo and 61 received ginkgo; 1 participant receiving placebo and 3 receiving ginkgo were lost to follow-up. Two serious adverse events (AEs) (myocardial infarction and severe depression) believed to be unrelated to the treatment occurred in the ginkgo group; otherwise, there were no significant differences in AEs. The differences (ginkgo - placebo) at exit in the z scores for the cognitive tests were as follows: PASAT -0.2 (95% confidence interval [CI] -0.5 to 0.1); Stroop Test -0.5 (95% CI -0.9 to -0.1); COWAT 0.0 (95% CI -0.2 to 0.3); and CVLT-II 0.0 (95% CI -0.3 to 0.3); none was statistically significant.
Conclusions: Treatment with ginkgo 120 mg twice a day did not improve cognitive performance in persons with MS.
Classification of evidence: This study provides Class I evidence that treatment with ginkgo 120 mg twice a day for 12 weeks does not improve cognitive performance in people with MS.
Figures
References
-
- Rao SM, Leo GJ, Bernardin L, Unverzagt F. Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction. Neurology 1991; 41: 685– 691 - PubMed
-
- Amato MP, Ponziani G, Siracusa G, Sorbi S. Cognitive dysfunction in early-onset multiple sclerosis: a reappraisal after 10 years. Arch Neurol 2001; 58: 1602– 1606 - PubMed
-
- Benedict RH, Cookfair D, Gavett R, et al. Validity of the minimal assessment of cognitive function in multiple sclerosis (MACFIMS). J Int Neuropsychol Soc 2006; 12: 549– 558 - PubMed
-
- Benedict RH, Zivadinov R. Risk factors for and management of cognitive dysfunction in multiple sclerosis. Nat Rev Neurol 2011; 7: 332– 342 - PubMed
-
- Harel Y, Appleboim N, Lavie M, Achiron A. Single dose of methylphenidate improves cognitive performance in multiple sclerosis patients with impaired attention process. J Neurol Sci 2009; 276: 38– 40 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials