

Preclinical assessment of comfort and secure fit of thermobrachytherapy surface applicator (TBSA) on volunteer subjects
- PMID: 22955650
- PMCID: PMC3439213
- DOI: 10.1120/jacmp.v13i5.3845
Preclinical assessment of comfort and secure fit of thermobrachytherapy surface applicator (TBSA) on volunteer subjects
Abstract
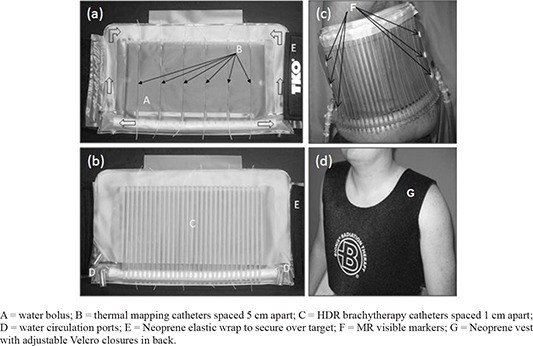
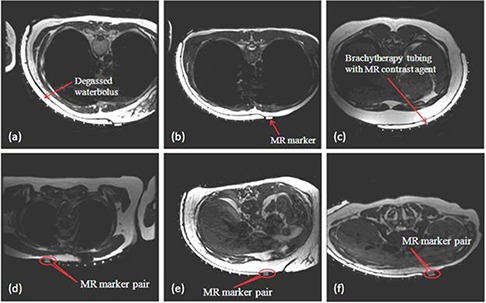
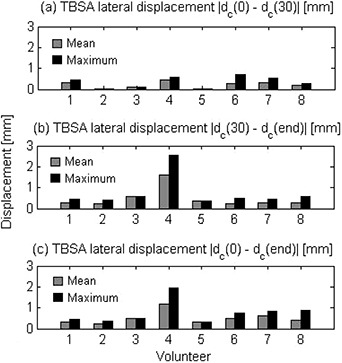
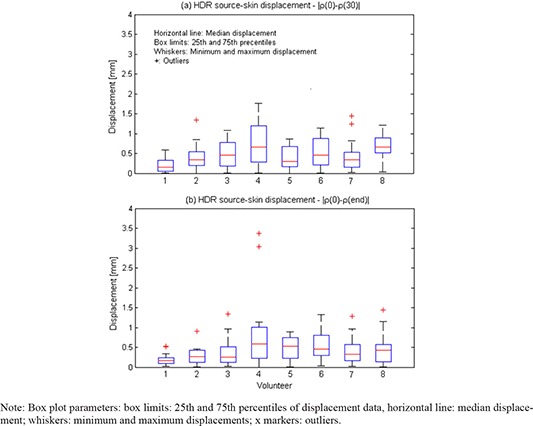
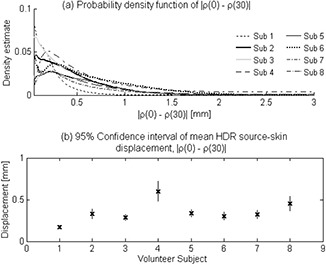
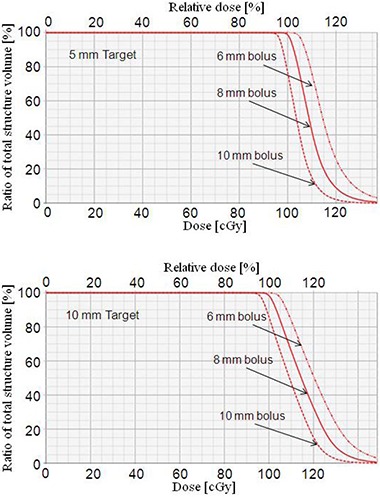
A thermobrachytherapy surface applicator (TBSA) was developed for simultaneous heat and brachytherapy treatment of chest wall (CW) recurrence of breast cancer. The ability to comfortably secure the applicator over the upper torso relative to the CW target throughout treatment is assessed on volunteers. Male and postmastectomy female volunteers were enrolled to evaluate applicator secure fit to CW. Female subjects with intact breast were also enrolled to assess the ability to treat challenging cases. Magnetic resonance (MR) images of volunteers wearing a TBSA over the upper torso were acquired once every 15 minutes for 90 minutes. Applicator displacement over this time period required for treatment preplanning and delivery was assessed using MR visible markers. Applicator comfort and tolerability were assessed using a questionnaire. Probability estimates of applicator displacements were used to investigate dosimetric impact for the worst-case variation in radiation source-to-skin distance for 5 and 10 mm deep targets spread 17 × 13 cm on a torso phantom. Average and median displacements along lateral and radial directions were less than 1.2 mm over 90 minutes for all volunteers. Maximum lateral and radial displacements were measured to be less than 1 and 1.5 mm, respectively, for all CW volunteers and less than 2 mm for intact breast volunteers, excluding outliers. No complaint of pain or discomfort was reported. Phantom treatment planning for the maximum displacement of 2 mm indicated < 10% increase in skin dose with < 5% loss of homogeneity index (HI) for -2 mm uniform HDR source displacement. For +2 mm uniform displacement, skin dose decreased and HI increased by 20%. The volunteer study demonstrated that such large and uniform displacements should be rare for CW subjects, and the measured variation is expected to be low for multifraction conformal brachytherapy treatment.
Figures


Similar articles
-
Thermal characteristics of thermobrachytherapy surface applicators for treating chest wall recurrence.Phys Med Biol. 2010 Apr 7;55(7):1949-69. doi: 10.1088/0031-9155/55/7/011. Epub 2010 Mar 12. Phys Med Biol. 2010. PMID: 20224154 Free PMC article.
-
Radiation dosimetry of a conformal heat-brachytherapy applicator.Technol Cancer Res Treat. 2004 Aug;3(4):347-58. doi: 10.1177/153303460400300404. Technol Cancer Res Treat. 2004. PMID: 15270585
-
Multilayer conformal applicator for microwave heating and brachytherapy treatment of superficial tissue disease.Int J Hyperthermia. 2006 Nov;22(7):527-44. doi: 10.1080/02656730600931815. Int J Hyperthermia. 2006. PMID: 17079212
-
Conformal microwave array (CMA) applicators for hyperthermia of diffuse chest wall recurrence.Int J Hyperthermia. 2010;26(7):686-98. doi: 10.3109/02656736.2010.501511. Int J Hyperthermia. 2010. PMID: 20849262 Free PMC article. Review.
-
Point: Hyperthermia with radiation for chest wall recurrences.J Natl Compr Canc Netw. 2007 Mar;5(3):339-44. doi: 10.6004/jnccn.2007.0029. J Natl Compr Canc Netw. 2007. PMID: 17439762 Review.
Cited by
-
Modelling Curved Contact Flexible Microstrip Applicators for Patient-Specific Superficial Hyperthermia Treatment Planning.Cancers (Basel). 2020 Mar 11;12(3):656. doi: 10.3390/cancers12030656. Cancers (Basel). 2020. PMID: 32168959 Free PMC article.
References
-
- Jones E, Oleson J, Prosnitz L, et al. Randomized trial of hyperthermia and radiation for superficial tumors. J Clin Oncol. 2005;23(13):3079–85. - PubMed
-
- Perez CA, Pajak T, Emami B, Hornback NB, Tupchong L, Rubin P. Randomized phase III study comparing irradiation and hyperthermia with irradiation alone in superficial measurable tumors. Final report by the Radiation Therapy Oncology Group. Am J Clin Oncol. 1991;14(2):133–41. - PubMed
-
- Sherar M, Liu FF, Pintilie M, et al. Relationship between thermal dose and outcome in thermoradiotherapy treatments for superficial recurrences of breast cancer: data from a phase III trial. Int J Radiat Oncol Biol Phys. 1997;39(2):371–80. - PubMed
-
- Vernon CC, Hand JW, Field SB, et al. Radiotherapy with or without hyperthermia in the treatment of superficial localized breast cancer: results from five randomized controlled trials. Int J Radiat Oncol Biol Phys. 1996;35(4):731–44. - PubMed
-
- Overgaard J. The current and potential role of hyperthermia in radiotherapy. Int J Radiat Oncol Biol Phys. 1989;16(3):535–49. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
