

Quality of life and survival in patients with advanced kidney failure managed conservatively or by dialysis
- PMID: 22956262
- PMCID: PMC3513739
- DOI: 10.2215/CJN.01130112
Quality of life and survival in patients with advanced kidney failure managed conservatively or by dialysis
Abstract
Background and objectives: Benefits of dialysis in elderly dependent patients are not clearcut. Some patients forego dialysis, opting for conservative kidney management (CKM). This study prospectively compared quality of life and survival in CKM patients and those opting for dialysis.
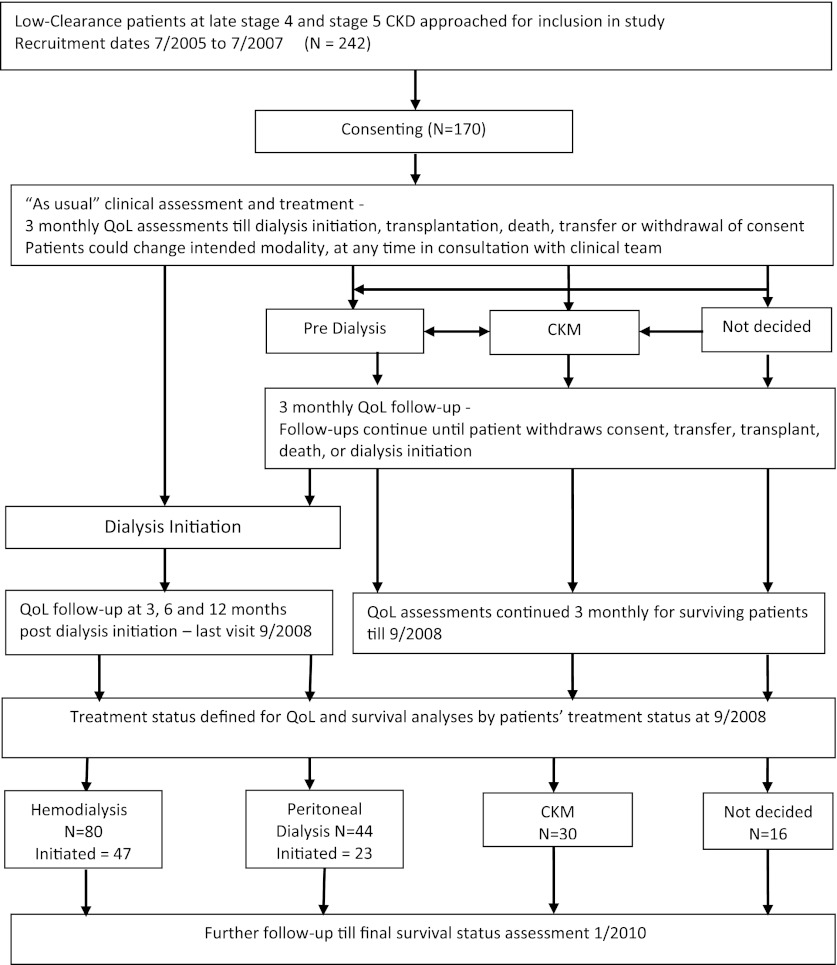
Design, setting, participants, & measurements: Quality-of-life assessments (Short-Form 36, Hospital Anxiety and Depression Scale, and Satisfaction with Life Scale) were performed every 3 months for up to 3 years in patients with advanced, progressive CKD (late stage 4 and stage 5).
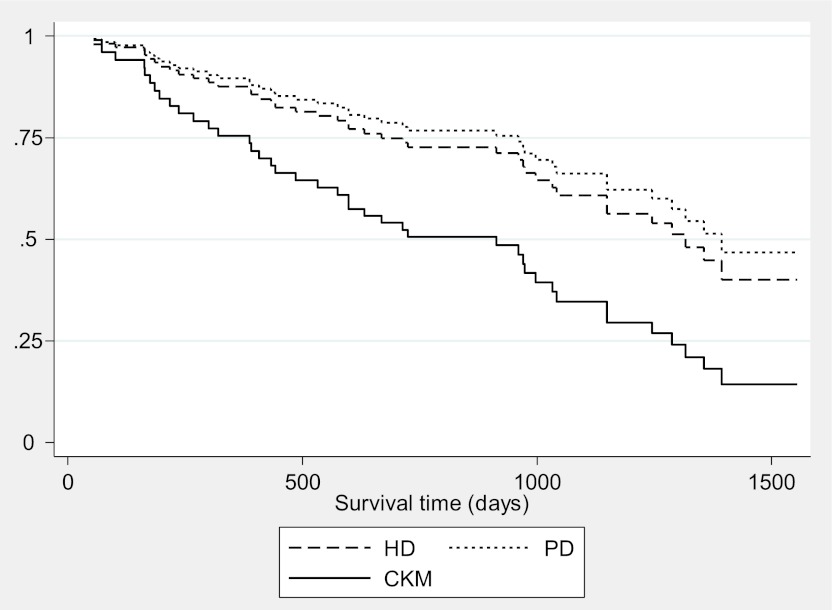
Results: After 3 years, 80 and 44 of 170 patients had started or were planned for hemodialysis (HD) or peritoneal dialysis, respectively; 30 were undergoing CKM; and 16 remained undecided. Mean baseline estimated GFR ± SD was similar (14.0 ± 4.0 ml/min per 1.73 m(2)) in all groups but was slightly higher in undecided patients. CKM patients were older, more dependent, and more highly comorbid; had poorer physical health; and had higher anxiety levels than the dialysis patients. Mental health, depression, and life satisfaction scores were similar. Multilevel growth models demonstrated no serial change in quality-of-life measures except life satisfaction, which decreased significantly after dialysis initiation and remained stable in CKM. In Cox models controlling for comorbidity, Karnofsky performance scale score, age, physical health score, and propensity score, median survival from recruitment was 1317 days in HD patients (mean of 326 dialysis sessions) and 913 days in CKM patients.
Conclusions: Patients choosing CKM maintained quality of life. Adjusted median survival from recruitment was 13 months shorter for CKM patients than HD patients.
Figures
Comment in
-
Deny dialysis or "D-NI" dialysis? The case for "do not initiate; do not ignore" orders.Clin J Am Soc Nephrol. 2012 Dec;7(12):1924-6. doi: 10.2215/CJN.11171012. Clin J Am Soc Nephrol. 2012. PMID: 23221096 No abstract available.
References
-
- Farrington K, Hodsman A, Casula A, Ansell D, Feehally J: UK Renal Registry 11th Annual Report (December 2008): Chapter 4 ESRD prevalent rates in 2007 in the UK: national and centre-specific analyses. Nephron Clin Pract 111[Suppl 1]: c43–c68, 2009 - PubMed
-
- Jager KJ, van Dijk PC, Dekker FW, Stengel B, Simpson K, Briggs JD, ERA-EDTA Registry Committee : The epidemic of aging in renal replacement therapy: An update on elderly patients and their outcomes. Clin Nephrol 60: 352–360, 2003 - PubMed
-
- Roderick P, Davies R, Jones C, Feest T, Smith S, Farrington K: Simulation model of renal replacement therapy: Predicting future demand in England. Nephrol Dial Transplant 19: 692–701, 2004 - PubMed
-
- Smith C, Da Silva-Gane M, Chandna S, Warwicker P, Greenwood R, Farrington K: Choosing not to dialyse: Evaluation of planned non-dialytic management in a cohort of patients with end-stage renal failure. Nephron Clin Pract 95: c40–c46, 2003 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
