

Greater complexity of liver surgery is not associated with an increased incidence of liver-related complications except for bile leak: an experience with 2,628 consecutive resections
- PMID: 22956403
- PMCID: PMC3855461
- DOI: 10.1007/s11605-012-2000-9
Greater complexity of liver surgery is not associated with an increased incidence of liver-related complications except for bile leak: an experience with 2,628 consecutive resections
Abstract
Background: Advances in technique, technology, and perioperative care have allowed for the more frequent performance of complex and extended hepatic resections. The purpose of this study was to determine if this increasing complexity has been accompanied by a rise in liver-related complications.
Methods: A large prospective single-institution database of patients who underwent hepatic resection was used to identify the incidence of liver-related complications. Liver resections were divided into an early era and a late era with equal number of patients (surgery performed before or after 18 May 2006). Patient characteristics and perioperative factors were compared between the two groups.
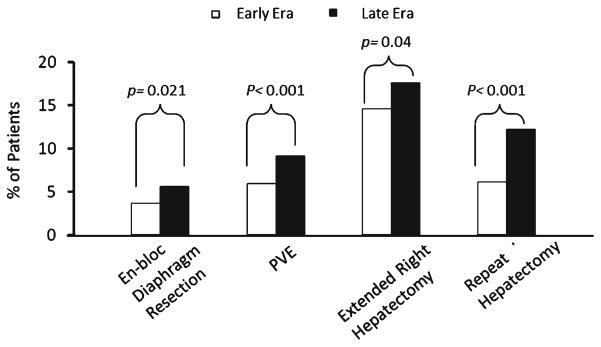
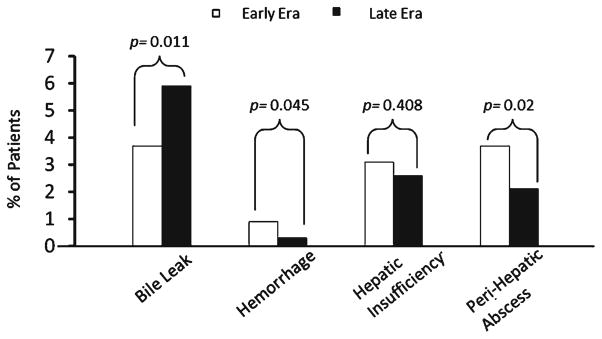
Results: Between 1997 and 2011, 2,628 hepatic resections were performed, with a 90-day morbidity and mortality rate of 37 and 2 %, respectively. We identified higher rates of repeat hepatectomy (12.2 vs 6.1 %; p < 0.001), two-stage resection (4.0 vs 1 %; p < 0.001), extended right hepatectomy (17.6 vs 14.6 %; p = 0.04), and preoperative portal vein embolization (9.1 vs 5.9 %; p < 0.001) in the late era. The incidence of perihepatic abscess (3.7 vs 2.1 %; p = 0.02) and hemorrhage (0.9 vs 0.3 %; p = 0.045) decreased in the late era and the incidence of hepatic insufficiency (3.1 vs 2.6 %; p = 0.41) remained stable. In contrast, the rate of bile leak increased (5.9 vs 3.7 %; p = 0.011). Independent predictors of bile leak included bile duct resection, extended hepatectomy, repeat hepatectomy, en bloc diaphragmatic resection, and intraoperative transfusion.
Conclusions: The complexity of liver surgery has increased over time, with a concomitant increase in bile leak rate. Given the strong association between bile leak and other poor outcomes, the development of novel technical strategies to reduce bile leaks is indicated.
Conflict of interest statement
Figures
References
-
- Palavecino M, Kishi Y, Chun YS, Brown DL, Gottumukkala VN, Lichtiger B, Curley SA, Abdalla EK, Vauthey JN. Two-surgeon technique of parenchymal transection contributes to reduced transfusion rate in patients undergoing major hepatectomy: analysis of 1,557 consecutive liver resections. Surgery. 2010;147:40–48. - PubMed
-
- Belghiti J, Hiramatsu K, Benoist S, Massault P, Sauvanet A, Farges O. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluate the actual risk of liver resection. J Am Coll Surg. 2000;191:38–46. - PubMed
-
- Vauthey JN, Chaoui A, Do KA, Bilimoria MM, Fenstermacher MJ, Charnsangavej C, Hicks M, Alsfasser G, Lauwers G, Hawkins IF, Caridi J. Standardized measurement of the future liver remnant prior to extended liver resection: methodology and clinical associations. Surgery. 2000;127:512–529. - PubMed
-
- Ribero D, Abdalla EK, Madoff DC, Donadon M, Loyer EM, Vauthey JN. Portal vein embolization before major hepatectomy and its effects on regeneration, resectability and outcome. Br J Surg. 2007;94:1386–1394. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
