

Elevated rheumatoid factor and long term risk of rheumatoid arthritis: a prospective cohort study
- PMID: 22956589
- PMCID: PMC3435445
- DOI: 10.1136/bmj.e5244
Elevated rheumatoid factor and long term risk of rheumatoid arthritis: a prospective cohort study
Abstract
Objective: To test whether elevated concentration of rheumatoid factor is associated with long term development of rheumatoid arthritis.
Design: A prospective cohort study, the Copenhagen City Heart Study. Blood was drawn in 1981-83, and participants were followed until 10 August 2010.
Setting: Copenhagen general population.
Participants: 9712 white Danish individuals from the general population aged 20-100 years without rheumatoid arthritis at study entry.
Main outcome measures: Rheumatoid arthritis according to baseline plasma IgM rheumatoid factor level categories of 25-50, 50.1-100, and >100, versus <25 IU/mL.
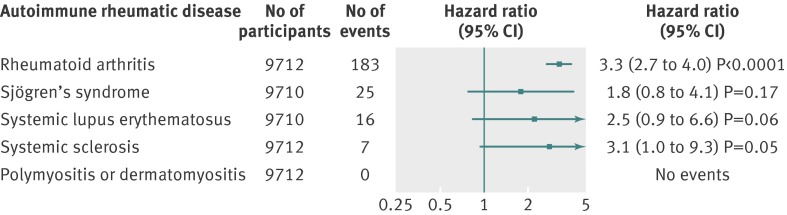
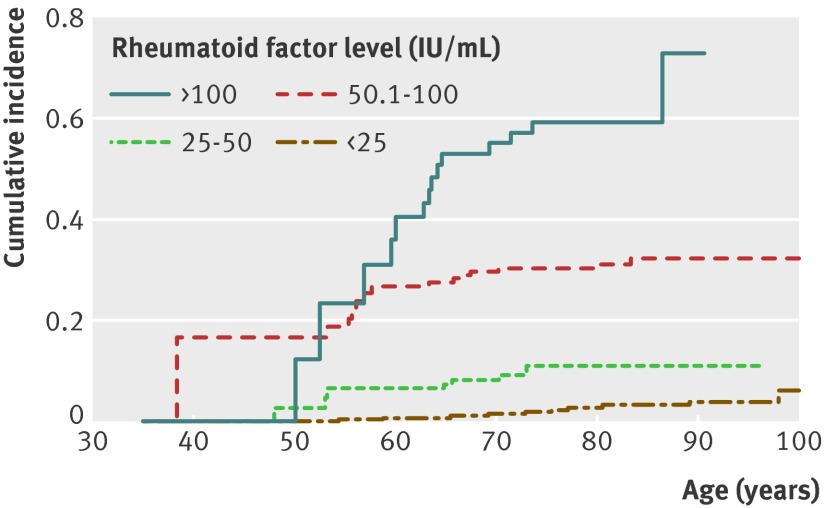
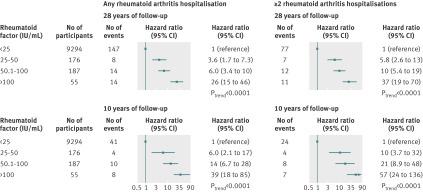
Results: Rheumatoid factor levels were similar from age 20 to 100 years. During 187,659 person years, 183 individuals developed rheumatoid arthritis. In healthy individuals, a doubling in levels of rheumatoid factor was associated with a 3.3-fold (95% confidence interval 2.7 to 4.0) increased risk of developing rheumatoid arthritis, with a similar trend for most other autoimmune rheumatic diseases. The cumulative incidence of rheumatoid arthritis increased with increasing rheumatoid factor category (P(trend)<0.0001). Multivariable adjusted hazard ratios for rheumatoid arthritis were 3.6 (95% confidence interval 1.7 to 7.3) for rheumatoid factor levels of 25-50 IU/mL, 6.0 (3.4 to 10) for 50.1-100 IU/mL, and 26 (15 to 46) for >100 IU/mL, compared with <25 IU/mL (P(trend)<0.0001). The highest absolute 10 year risk of rheumatoid arthritis of 32% was observed in 50-69 years old women who smoked with rheumatoid factor levels >100 IU/mL.
Conclusion: Individuals in the general population with elevated rheumatoid factor have up to 26-fold greater long term risk of rheumatoid arthritis, and up to 32% 10 year absolute risk of rheumatoid arthritis. These novel findings may lead to revision of guidelines for early referral to a rheumatologist and early arthritis clinics based on rheumatoid factor testing.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures


Comment in
-
Rheumatoid factor positivity in the general population.BMJ. 2012 Sep 6;345:e5841. doi: 10.1136/bmj.e5841. BMJ. 2012. PMID: 22956591 No abstract available.
-
Rheumatoid arthritis: RF levels predict RA risk in the general population.Nat Rev Rheumatol. 2012 Oct;8(10):562. doi: 10.1038/nrrheum.2012.159. Epub 2012 Sep 18. Nat Rev Rheumatol. 2012. PMID: 22986461 No abstract available.
References
-
- Gaston JSH. Rheumatic diseases, immunological mechanisms and prospects for new therapies. University of Cambridge, 1999.
-
- Neovius M, Simard JF, Askling J. Nationwide prevalence of rheumatoid arthritis and penetration of disease-modifying drugs in Sweden. Ann Rheum Dis 2011;70:624-9. - PubMed
-
- Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism Collaborative initiative. Arthritis Rheum 2010;62:2569-81. - PubMed
-
- Cohen SB. Targeting the B cell in rheumatoid arthritis. Best Pract Res Clin Rheumatol 2010;24:553-63. - PubMed
-
- Don BR, Kim K, Li J, Dwyer T, Alexander F, Kaysen GA. The effect of etanercept on suppression of the systemic inflammatory response in chronic hemodialysis patients. Clin Nephrol 2010;73:431-8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical