

Tight glycemic control versus standard care after pediatric cardiac surgery
- PMID: 22957521
- PMCID: PMC3501680
- DOI: 10.1056/NEJMoa1206044
Tight glycemic control versus standard care after pediatric cardiac surgery
Abstract
Background: In some studies, tight glycemic control with insulin improved outcomes in adults undergoing cardiac surgery, but these benefits are unproven in critically ill children at risk for hyperinsulinemic hypoglycemia. We tested the hypothesis that tight glycemic control reduces morbidity after pediatric cardiac surgery.
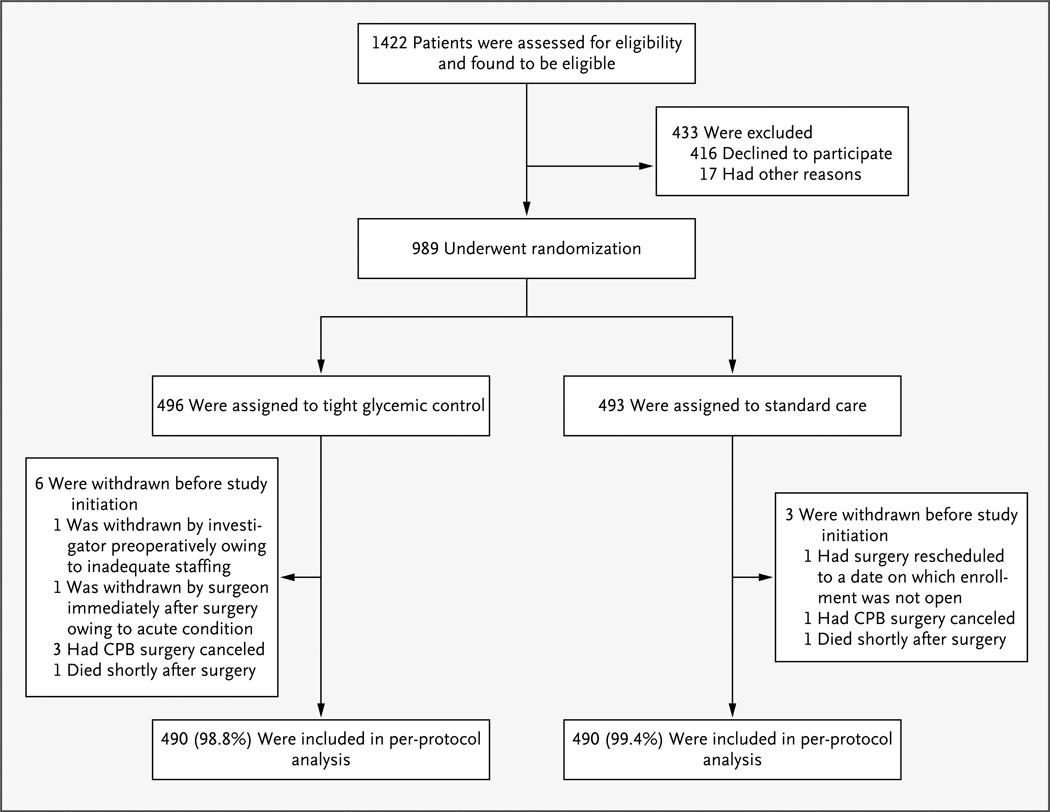
Methods: In this two-center, prospective, randomized trial, we enrolled 980 children, 0 to 36 months of age, undergoing surgery with cardiopulmonary bypass. Patients were randomly assigned to either tight glycemic control (with the use of an insulin-dosing algorithm targeting a blood glucose level of 80 to 110 mg per deciliter [4.4 to 6.1 mmol per liter]) or standard care in the cardiac intensive care unit (ICU). Continuous glucose monitoring was used to guide the frequency of blood glucose measurement and to detect impending hypoglycemia. The primary outcome was the rate of health care-associated infections in the cardiac ICU. Secondary outcomes included mortality, length of stay, organ failure, and hypoglycemia.
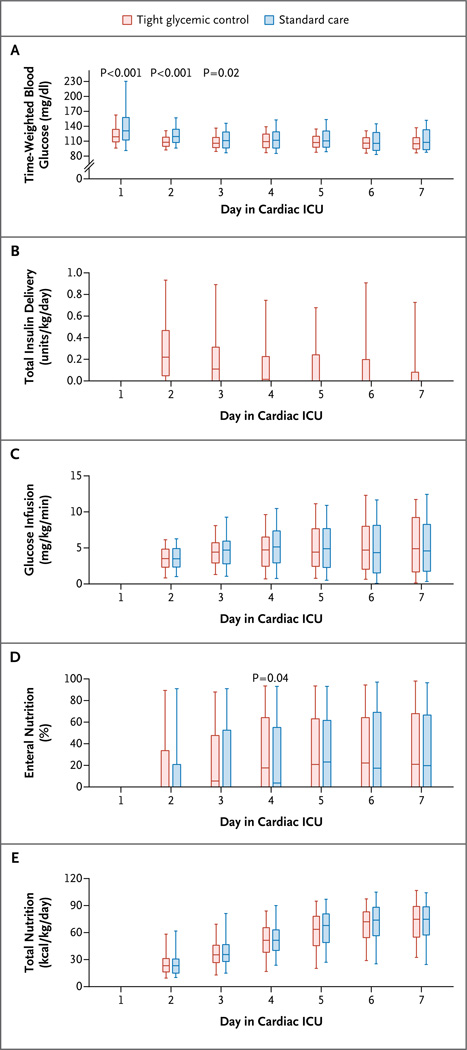
Results: A total of 444 of the 490 children assigned to tight glycemic control (91%) received insulin versus 9 of 490 children assigned to standard care (2%). Although normoglycemia was achieved earlier with tight glycemic control than with standard care (6 hours vs. 16 hours, P<0.001) and was maintained for a greater proportion of the critical illness period (50% vs. 33%, P<0.001), tight glycemic control was not associated with a significantly decreased rate of health care-associated infections (8.6 vs. 9.9 per 1000 patient-days, P=0.67). Secondary outcomes did not differ significantly between groups, and tight glycemic control did not benefit high-risk subgroups. Only 3% of the patients assigned to tight glycemic control had severe hypoglycemia (blood glucose <40 mg per deciliter [2.2 mmol per liter]).
Conclusions: Tight glycemic control can be achieved with a low hypoglycemia rate after cardiac surgery in children, but it does not significantly change the infection rate, mortality, length of stay, or measures of organ failure, as compared with standard care. (Funded by the National Heart, Lung, and Blood Institute and others; SPECS ClinicalTrials.gov number, NCT00443599.).
Figures
Comment in
-
Glucose in the ICU--evidence, guidelines, and outcomes.N Engl J Med. 2012 Sep 27;367(13):1259-60. doi: 10.1056/NEJMe1209429. Epub 2012 Sep 7. N Engl J Med. 2012. PMID: 22957522 No abstract available.
-
Glucose in the ICU--evidence, guidelines, and outcomes.N Engl J Med. 2012 Dec 20;367(25):2451-2; author reply 2452-3. doi: 10.1056/NEJMc1212933. N Engl J Med. 2012. PMID: 23252538 No abstract available.
-
Glucose in the ICU--evidence, guidelines, and outcomes.N Engl J Med. 2012 Dec 20;367(25):2452; author reply 2452-3. doi: 10.1056/NEJMc1212933. N Engl J Med. 2012. PMID: 23252539 No abstract available.
References
-
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–1900. - PubMed
-
- O’Brien SM, Clarke DR, Jacobs JP, et al. An empirically based tool for analyzing mortality associated with congenital heart surgery. J Thorac Cardiovasc Surg. 2009;138:1139–1153. - PubMed
-
- Malmberg K, Rydén L, Efendic S, et al. Randomized trial of insulin-glucose infusion followed by subcutaneous insulin treatment in diabetic patients with acute myocardial infarction (DIGAMI study): effects on mortality at 1 year. J Am Coll Cardiol. 1995;26:57–65. - PubMed
-
- Van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU. N Engl J Med. 2006;354:449–461. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical