

Validation of CRP as prognostic marker for renal cell carcinoma in a large series of patients
- PMID: 22958305
- PMCID: PMC3502607
- DOI: 10.1186/1471-2407-12-399
Validation of CRP as prognostic marker for renal cell carcinoma in a large series of patients
Abstract
Background: To evaluate the prognostic significance of the pre-operative C-reactive protein (CRP) serum level in patients with renal cell cancer (RCC).
Methods: We evaluated 1,161 RCC patients with complete patient and tumour specific characteristics as well as information about their pre-operative CRP-level, who had undergone either radical nephrectomy or nephron-sparing surgery at two German high-volume centres (University Hospitals of Hannover and Ulm). The mean follow-up was 54 months.
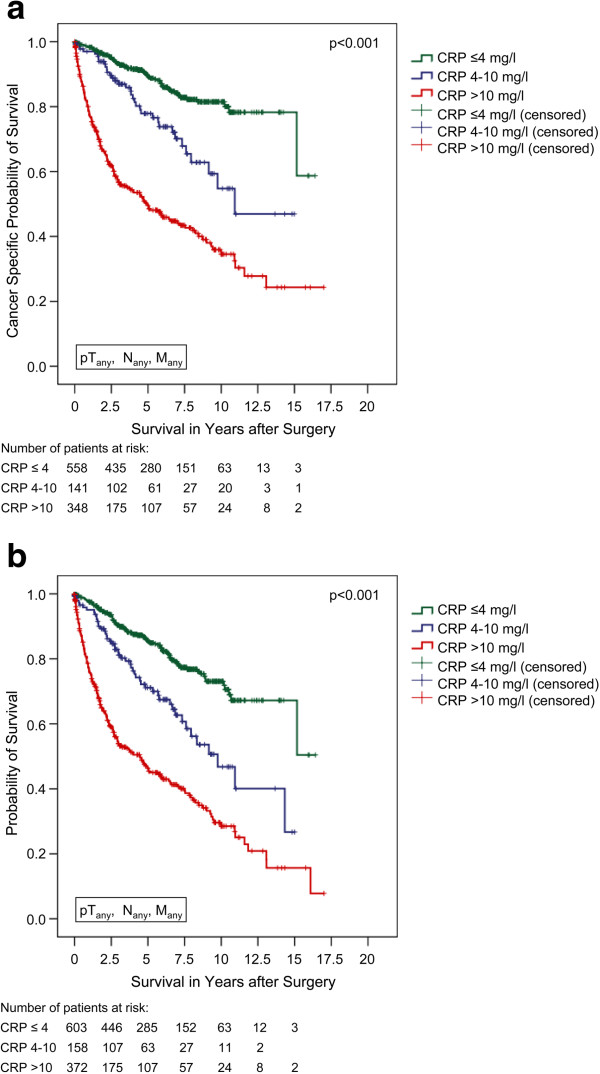
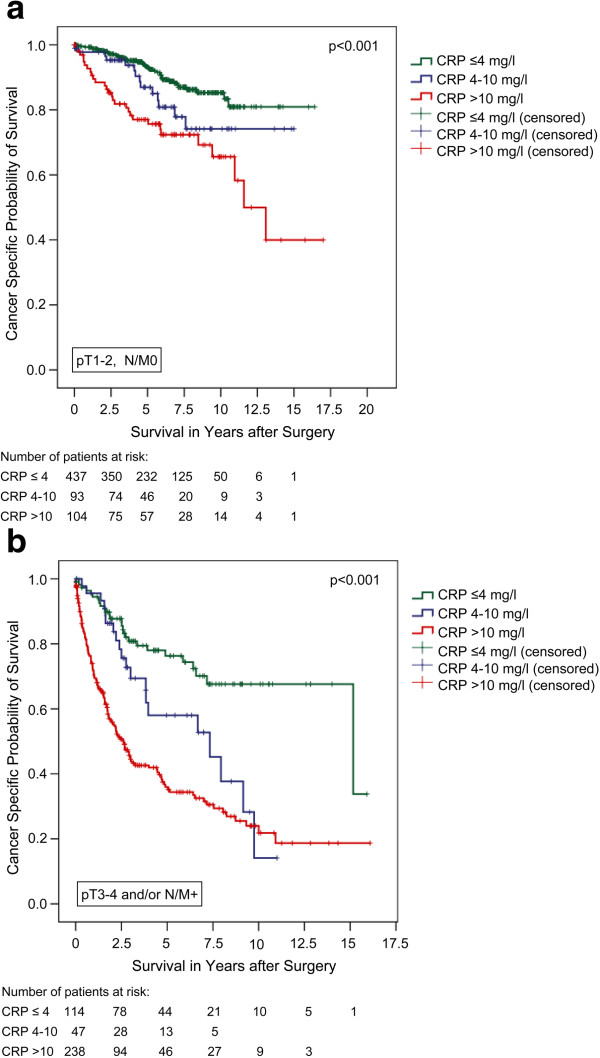
Results: The CRP-level, stratified to three subgroups (CRP ≤ 4, 4-10, and >10 mg/l), correlated significantly with tumour stage (p < 0.001), the risk of presenting nodal disease (2.1, 3.1, and 16.4%) and distant metastasis (2.9, 8.6, and 30.0%; p < 0.001). The Kaplan-Meier 5-year cancer specific survival (CSS) rates were 89.4, 77.9, and 49.5%, respectively (p < 0.001). Multivariate analysis identified CRP as an independent prognosticator for CSS as well as overall survival (p < 0.001). Patients with a CRP of 4-10 and >10 mg/l had a 1.67 and 2.48 fold higher risk of dying due to their RCC compared to those with a pre-operative CRP ≤4 mg/l, respectively.
Conclusions: A high preoperative serum CRP level is an independent predictor of poor survival in patients with RCC. Its routine use could allow better risk stratification and risk-adjusted follow-up of RCC patients.
Figures
References
-
- Ljungberg B. Prognostic factors in renal cell carcinoma. Der Urologe Ausg. 2004;43(Suppl 3):119–120. - PubMed
-
- Kozlowski JM. Management of distant solitary recurrence in the patient with renal cancer. Contralateral kidney and other sites. Urol Clin North Am. 1994;21:601–624. - PubMed
-
- Rabinovitch RA, Zelefsky MJ, Gaynor JJ, Fuks Z. Patterns of failure following surgical resection of renal cell carcinoma: implications for adjuvant local and systemic therapy. J Clin Oncol. 1994;12:206–212. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
