

Role of quantitative CT in predicting postoperative FEV1 and chronic dyspnea in patients undergoing lung resection
- PMID: 22958356
- PMCID: PMC3463043
- DOI: 10.1186/2049-6958-5-3-188
Role of quantitative CT in predicting postoperative FEV1 and chronic dyspnea in patients undergoing lung resection
Abstract
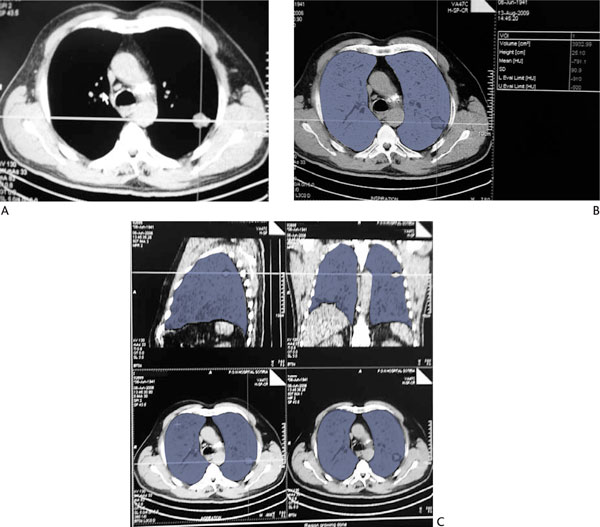
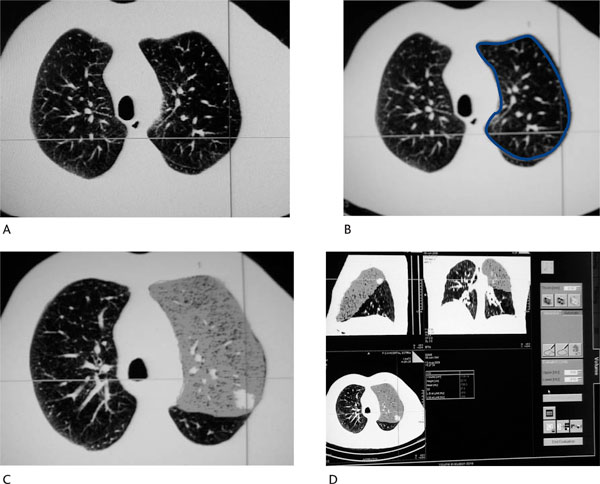
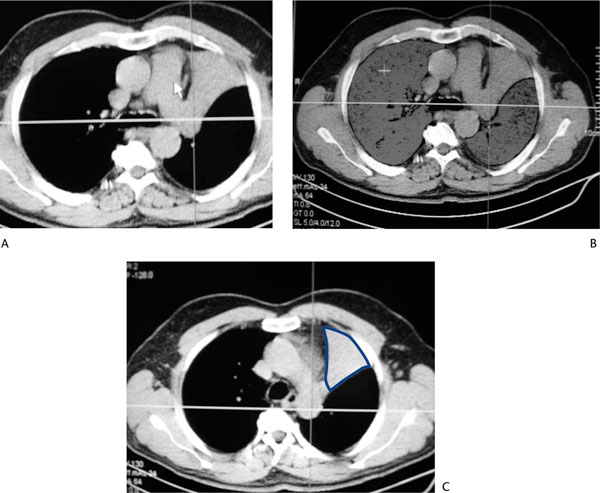
Lung resection is the mainstay of treatment in patients with early stage non-small cell lung cancer. However, lung cancer patients often suffer from comorbidities and the respiratory reserve should be carefully evaluated preoperatively in order to avoid postoperative complications. Forced expiratory volume in 1 second (FEV1) is considered to be an index that depicts the patient's respiratory efficacy and its prediction has a key role in the preoperative evaluation of lung cancer patients with impaired lung function. Prediction of postoperative FEV1 is currently possible with the use of perfusion radionuclide lung scanning.Quantitative CT is the analysis of data acquired during normal chest CT scan using the system's software. By applying a dual threshold of -500 to -910 Hounsfield Units, functional lung volumes are estimated and postoperative FEV1 can be predicted by reducing the preoperative measurement by the fraction of the part to be resected.Studies have shown that preoperative predictions correlate well with the actual postoperative measurements. Additionally, quantitative CT results are in good agreement with perfusion scintigraphy predictions. Newer radiological techniques such as perfusion MRI and co-registered SPECT/CT have also been used in the preoperative evaluation with similar results.In conclusion, chest CT which is obligatory for staging, can be used for quantitative analysis of the already available data. It is technically simple, providing an accurate prediction of postoperative FEV1. Thus, quantitative CT appears to be a useful tool in the preoperative evaluation of lung cancer patients undergoing lung resection.
Figures
References
-
- Brunelli A, Charloux A, Bolliger CT, Rocco G, Sculier JP, Varela G, Licker M, Ferguson MK, Faivre-Finn C, Huber RM, Clini EM, Win T, De Ruysscher D, Goldman L. European Respiratory Society and European Society of Thoracic Surgeons joint task force on fitness for radical therapy. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy) Eur Respir J. 2009;34:17–41. doi: 10.1183/09031936.00184308. - DOI - PubMed
-
- Markos J, Mullan BP, Hillman DR, Musk AW, Antico VF, Lovegrove FT, Carter MJ, Finucane KE. Preoperative assessment as a predictor of mortality and morbidity after lung resection. Am Rev Respir Dis. 1989;139:902–910. - PubMed
-
- Beckles MA, Spiro SG, Colice GL, Rudd RM. The physiologic evaluation of patients with lung cancer being considered for resectional surgery. Chest. 2003;123(1 Suppl):105S–114S. - PubMed
LinkOut - more resources
Full Text Sources
